Over the weekend, I was unfortunate enough to come across an article by Jaclyn Harwell at “Modern Alternative Health” called “5 Reasons That Measles is Better Than Autism.” Unsurprisingly, it was full of misinformation and shoddy arguments. Indeed, it was so full of counterfactual claims and dishonest distortions of reality that I felt compelled to write a rebuttal, especially since the faulty arguments contained in the post are prevalent among antivaccers. Therefore, I am going to dissect that post and explain why it is nonsense. Before I get to Jaclyn’s “5 reasons,” however, I need to deal with several serious problems in the opening statements of the article.
First, this post is fundamentally flawed because the entire thing is based on the false dichotomy that you have to choose between because vaccines and autism. In reality, of course, vaccines do not cause autism. As I explained at length in this post, numerous enormous studies have tested the vaccine/autism hypothesis and failed to find any evidence of vaccines causing autism. The only studies that suggested that vaccines cause autism were tiny and riddled with problems. Anecdotes don’t matter, deceptive documentaries are irrelevant, and the “CDC whistle-blower” did not present any actual evidence of vaccines causing autism (or of CDC corruption, for that matter). Only scientific evidence matters, and science is overwhelmingly on the side of vaccines.

Second, the core argument throughout the article is that measles is a mild illness, but that argument is a blatant lie. I’ll deal with this at length under reason #5, but briefly, in developed countries with access to modern medicine, measles still has a death rate of 1 in 1,000 infected individuals. Nevertheless, it is true that in terms of sheer numbers, there are few measles deaths in industrialized countries today, but that is only because of vaccines! Indeed, in the US, in the 10 years prior to the introduction of the measles vaccine, measles killed an average of 440.3 children each year in the US alone (details and sources here; also note that the death rate per infected individual was roughly 1 in 1,000 then as well). Further, when we look at the entire world, measles still kills well over 100,000 people annually, and the World Health Organization describes it as, “one of the leading causes of death among young children” (WHO 2016). That’s not fear-mongering, that’s a fact. So while anti-vaccers want you to think that measles is trivial, actual epidemiologists have a very different view of this disease.
Further, even when children don’t die from measles, there is still a 1 in 10 chance that they will develop an ear infection (which can cause permanent hearing loss), a 1 in 20 chance that they will develop pneumonia, and a 1 in 1,000 chance that they will develop encephalitis (a swelling of the brain; CDC 2015a). There are also other complications such as febrile seizures in 0.1–2.3% of patients (Orenstein et al. 2004). Indeed, during a large outbreak in France, nearly 25% of victims had to be hospitalized (Antona et al. 2013), and in the US from 2001–2008, 40% of measles patients were hospitalized (CDC 2011). You simply cannot describe a disease that hospitalizes 25–40% of its victims and kills over 100,000 people annually as a minor illness (WHO 2016). That is extremely dishonest (see reason #5 for a more thorough explanation of just how deadly this disease truly is).

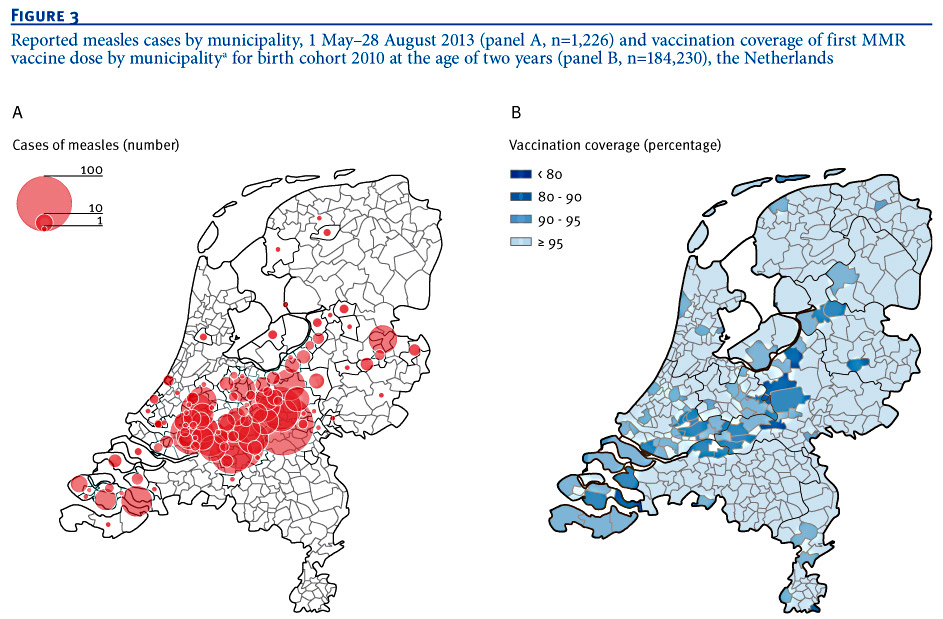
Please carefully note how the measles outbreaks are centered around the communities with low vaccination rates. Image from Knol et al. 2013
Third, the author claims that, “in the majority of outbreaks, most affected people have, indeed, been vaccinated.” This is an extremely common anti-vaccine argument, and it is horribly flawed. First, in the case of measles the claim itself isn’t even true. For example, in the 2001–2008 study that I mentioned earlier, 89% of patients were unvaccinated (CDC 2011). Similarly, during an enormous outbreak in France that involved over 20,000 people, 80% of patients were unvaccinated (Antona et al. 2013), and during a large outbreak in the Netherlands, 91.7% of patients were unvaccinated (Knol et al. 2013). Those are not cherry-picked examples. Rather they are the norm for measles outbreaks.
Additionally, and far more importantly, this argument ignores rudimentary math. You have to look at the proportions not the raw numbers. Most people are vaccinated, so of course many outbreaks will affect vaccinated people. Simply looking at the raw number of cases doesn’t tell us whether or not vaccinated people actually get the disease more often, and when we look at the actual rates, we find that infection rates are substantially higher among the unvaccinated (King et al. 1991; Schmitz et al. 2011). To give a completely analogous example, most car accidents involve sober drivers, but that doesn’t mean that driving drunk isn’t dangerous. Most people drive sober. Therefore, in terms of raw numbers, most accidents involve sober drivers. However, when you look at the rates, you find that the rate of accidents is far higher among drunk drivers than among sober drivers.
Finally, the author insinuates that “the efficacy of vaccinations is questionable at best.” Again, this is simply not true, especially for the measles vaccine. Even beyond the examples that I cited early of outbreaks corresponding to unvaccinated communities and higher measles rates among the unvaccinated, many other studies have examined the efficiency of the measles vaccine and it is quite high (93% with one dose and 95–97% with two doses; King et al. 1991; CDC 2015b). For example, Clemens et al. (1988), found that introducing the measles vaccine into a population reduced the measles death rates by 57%, but please go ahead and say that the vaccine isn’t effective or important (note the immense sarcasm).
Now that we are clear on the actual facts, let’s look at the five arguments in the article. My intention is to address the original article point by point, but the original jumped around quite a bit and didn’t follow a great logical structure. As a result, I thought that it might be useful to provide a bullet list of key points and the sections in which they are discussed.
- Vaccines don’t cause autism (introduction, #1)
- Getting measles to avoid getting measles is idiotic (#1)
- Measles actually weakens the immune system (#2)
- Neither measles nor autism can be cured, but measles can be prevented (#4)
- Total measles mortalities are relatively low because of vaccines (#1, #5)
- Measles still kills over 100,000 people annually (introduction, #1, #5)
- Without vaccines measles would kill over 1 million people annually (#5)
- Without vaccines, at least 0.35 in 100 children under the age of five would die from measles each year (#5)
Note: To be clear, if you want to say that surviving a measles infection without any serious or lasting consequences is better than a life-long affliction with severe autism, fine, I’m not going to disagree with you. What I take issue with is the dishonest and misleading claims about measles mortality rates, the dangerous and unmerited vilification of vaccines, and the damaging way that autism is presented. We need to stop talking about autism as if it is the world’s worst disease and as if people with autism are inferior, damaged, and in need of repair. That is an indignity that autistic people should not have to suffer. Autism is not the worst thing that could happen to your child.
Bad reason #1: “Measles imparts lifelong immunity.”
I have repeatedly had to address this argument from anti-vaccers (for example here and here), which is frustrating because it is such an obviously ridiculous argument. We can rephrase this argument simply as, “getting measles is good because it prevents you from getting measles.” Think about that for a second. This argument i
s actually proposing that you should avoid getting sick by getting sick. In contrast, a vaccine will prevent you from ever getting sick. In other words, a vaccine prevents you from ever getting measles, whereas measles only prevents you from getting measles a second time. Using a measles infection to protect you from a measles infection is like using pregnancy as a contraceptive.
To be fair, some studies have found that vaccine-induced immunity does not last as long as natural immunity (Christenson and Bottiger 1994), but other research has found that both forms last equally well for many years (Jokinen et al. 2007), and since measles is predominantly a childhood disease, those first years are the really important ones. Additionally, the longevity of immunity can easily, safely, and effectively be extended with boosters, which, once again, prevent you from getting measles in the first place. Further, I have already provided multiple citations showing that the measles vaccine is very effective and infection rates are much higher among the unvaccinated. In other words, this anti-vaccine argument makes it sound like getting measles is the best way to avoid getting measles, but that is clearly ridiculous. The vaccine is by far the best way to avoid ever having to suffer through measles.
Jaclyn goes on to reiterate that measles “isn’t a big deal” by citing the fact that between 1950 and 1960 the death rate for the US was less than 1 per 100,000 individuals (for the entire population, not per infected individual). As I showed earlier, however, that comes out to well over 400 deaths annually, which is in fact a big deal (also see #5 for an explanation of why the 1 in 100,000 figure is misleading). Even if vaccines caused autism (which again, they don’t), a life of autism is not worse than death by measles.
She also claims that there were no deaths among the 1,153 US cases of measles from 2001–2013. First, that claim is not true. There were two measles deaths from 2001–2003 (CDC 2004), another two in 2009 (Kockanek 2011), and another two in 2010 (Murphy 2010). Nevertheless, the death rates are low, but this argument totally ignores the fact that the reason that we have so few deaths is because we have so few cases of measles, and the reason that we have so few cases is because we have vaccines! Vaccines are the only reason that we don’t have thousands of measles deaths each year. Indeed, it is estimated that between 1994 and 2013, the measles vaccine prevented >70 million cases of measles in the US, which comes out to a total of 57,300 deaths according to the calculations used by the authors (Whitney et al. 2014). That number may, however, be higher. If, for example, we simply apply the normally accepted 1 in 1000 death rate, then it would be 70,000 deaths (3,500 measles induced deaths annually). Either way, the point is that the vaccine prevents thousands of deaths each year, and you simply cannot pass that off as a minor thing.
Finally, she quotes a “study” which said that, “The mass of scientific evidence compiled by researchers clearly indicates that the incidence of autism occurs following vaccination and is most closely associated with the schedule of vaccines culminating in the MMR vaccine” (Ewing 2009). However, that “study” was not actually a study. It wasn’t even a proper review. It was an entirely speculative opinion piece that made one false claim and unmerited assumption after another. It was based on a correlation fallacy, and it never once provided actual evidence to support the quoted statement. Further, it ignored the vast body of large studies that failed to find any evidence of vaccines causing autism. In other words, all that this paper did was propose a hypothesis, but that hypothesis has already been thoroughly tested and falsified.
Indeed, even the first sentence of the paper is demonstrably false. It says, “that the occurrence of autism has risen steadily in the last decades is not in dispute.” In reality, the rise in autism rates is very much in dispute, with many studies concluding that it is at least largely due to a change in diagnostic criteria rather than an actual increase (Rutter 2005; Taylor 2006; Bishop et al. 2008; Baxter et al. 2015; Hansen et al. 2015). When I first looked at this paper, I was baffled by how a paper that opened with such a clearly false statement could possibly have passed peer-review. Then, I checked the journal it was published in, and it was a journal that that is so minor that it doesn’t even have an impact factor (in other words, the scientific community doesn’t take it very seriously). You should always be wary of journals like this.
Bad reason #2: “Measles strengthens the immune system.”
No it doesn’t. I explained this in detail here, but in short, after a measles infection, your body produces antibodies that are specific for measles. So it only “strengthens” your immune system in that you can’t get measles again. It doesn’t help you fight any other infections. Further, as I explained under #1, thanks to vaccines, you can get those exact same antibodies without actually getting measles.
Further, recent research has shown that measles infections are so hard on your immune system that it actually takes up to 2–3 years for a child’s immune system to return to normal functional levels (Mina et al. 2015). In other words, measles infections weaken the immune system for several years, and these weakened immune systems lead to infections and deaths that aren’t generally attributed to measles. As a result, the actual measles death tolls are higher than we realize (not to mention that these additional infections often come with lasting side-effects).
Finally, it is true that associations with some microorganisms help to prevent autoimmune disorders, but that is actually because those organisms “train” the immune system not to over-react. So they aren’t “strengthening” the immune system, they are training it give a reduced response (a “strengthened” or “boosted” immune system is actually what causes autoimmune disorders). Further, the microbes that do this are generally beneficial or benign, not pathogenic (Gaurner et al. 2006). So there is no evidence that a measles infection will help you out later down the road.
Bad reason #3: “Autism causes long-term damage.”
I certainly don’t deny that autism can cause life long-problems (though I would like to stress that autism is a spectrum of disorders, and many people who are clinically diagnosed as autistic are very high functioning and live normal lives). However, in this section, Jaclyn reiterates her claims that measles isn’t dangerous, a measles infection gives life-long immunity to measles, etc. This section is really just a rehash of previous sections, so I won’t belabor the point.
Bad reason #4: “Measles is easier to cure than autism.”
I’m not arguing against the core statement here, but the pseudoscience that she uses to try to back up that statement is deplorable. For example, she opens with, “There’s actually no cure for measles. Know why? Because it’s a benign childhood disease” (her emphasis). First, there is no cure because it is a viral infection, and they are notoriously hard to cure (that is why we are also lacking cures for HIV, H1N1, the common cold, etc.). Second, another reason that there is no cure is that most people aren’t looking for a cure, because we have vaccines. In other words, we know that vaccines work very well, so it is more effective to invest money in increasing vaccine coverage, rather than in looking for a cure. Third, once again, measles has a death toll of over 100,000 people annually, and, as I’ll explain in #5, without vaccines that number would be well over 1,000,000. You simply cannot describe that as “benign.”
Next, she further tries to downplay the severity of measles by claiming that treatment with vitamin A reduces death rates by 62%. You’d think that the fact that she is talking about reducing death rates would make her rethink her claim that measles is “benign,” but apparently not. Nevertheless, there is some evidence that vitamin A is useful in overcoming a measles infection. However, citing that 62% figure without context is very deceptive, because it comes from a meta-analysis of studies in Africa where vitamin A deficiencies are major problems (Sudfeld et al. 2010). In industrialized counties, however, most of us have plenty of vitamin A, and vitamin A is a standard part of measles treatments (CDC 2016a). In other words, that 1 in 1,000 death rate that we talked about early already includes vitamin A treatments, but if you read Jaclyn’s post, it sounds like vitamin A is a way for you to improve those odds.
Finally, she claims that autism can be cured, which is a dangerous way to give parents false hope. There is currently no cure for autism (after all, it’s largely genetic). There are ways to help manage it, but not cure it (please don’t flood the comments with anecdotes, because anecdotes are not valid scientific evidence. If you don’t have large, properly controlled clinical trials that were published in reputable journals, then you don’t have any evidence).
Note: If you want to be pedantic, neither measles nor autism can be “cured” because your body, not a medication, is actually what fights the measles infection. So if we are going to succumb to pedantry, the core claim of this argument isn’t technically true.
Bad reason #5: “Measles complications are uncommon.”
Much of this section is a regurgitation of previous arguments, so I will focus on the novel parts. The first of which is the claim that 1 in 45 children in the US have autism, coupled with the claim that 1% of the entire world’s population is autistic. I don’t have too much trouble with the 1 in 45 claim because it came from a legitimate study (though it is worth noting that the estimate that is currently accepted by health organizations is actually 1 in 68 children in the US; CDC 2016b), but the 1% figure is misleading. No source is given, but the source that I found lists it as 0.6%, not 1%, and when we are dealing with the world’s entire population, that rounding error is substantial (roughly 28 million people; Elsabbagh et al. 2012). Also, I have a serious problem with the way that those numbers are being used here. Jaclyn is clearly trying to use them to argue that autism is a very common thing, and, therefore, should be feared. However, autism is a spectrum of disorders, and early in the post, Jaclyn said that her post was “referring to children with severe, regressive cases of autism, not those that are high-functioning and more self-sufficient.” Do you see the problem? It is extremely dishonest to cite the overall autism rate if you are only talking about the most extreme versions of it. In other words, 0.6% of the world’s population has some form of autism, but only a small subset of that 0.6% has the type of severe autism that this post was supposedly about. So this is yet another instance of her using numbers dishonestly in a failed attempt to support her flawed position.
Next, she makes the argument that most measles deaths are actually from developing countries that have poor sanitation standards. The claim itself is true, but the insinuation that sanitation standards are the cause of the infections is false. The deaths are from those countries because they are the ones that don’t have vaccines. As I explained here and here, the sanitation standards in the US were essentially the same in the 50s as they are now, yet they still had hundreds of measles deaths each year. Why? Because they didn’t have vaccines. Similarly, when we introduce vaccines into countries with very poor sanitation standards, the death rates drop (Clemens et al. 1988). Why? Because vaccines work (King et al. 1991; CDC 2015b). Further, as I explained earlier, industrialized countries continue to have large measles outbreaks when vaccination rates drop, and some of those outbreaks result in unnecessary deaths (Antona et al. 2013; Knol et al. 2013).
She then goes on to act as if the 100,000+ annual deaths from measles aren’t really a big deal because they only represent a small portion of the total population. First, I find that attitude unconscionable, since those deaths are preventable. Second, vaccines are the only reason that the death rate is so low! Even if we back the clock up to the year 2000, the death toll was 546,800 (WHO. 2016). Why did it drop so rapidly between then and now? Because we have had a massive vaccination campaign and have taken vaccines to many developing countries, including ones that lack sanitation. Indeed, it is estimated that between 2000 and 2014, the measles vaccine prevented over 17.1 million deaths (WHO 2016). That’s 1.14 million per year. So you simply cannot present the current number of mortalities as evidence that we shouldn’t vaccinate, because the current numbers are low because of vaccines.
Additionally, there is a huge problem here because the autism rates and measles death rates aren’t exactly comparable. For example, she claims that 1% of the world’s population has autism (that should be 0.6%), whereas only 0.002% of the world’s population dies from measles each year. Her argument seems to be that the odds of having autism are far greater than the odds of dying of measles, but that is not a fair comparison because measles deaths are not distributed evenly by age, and roughly 55% of deaths occur in children under 5 (Orenstein et al. 2004). So when you want to look at risk, you can’t simply divide the death rate by the world’s entire population (as she did) because children that die at a young age aren’t recruited into the older age groups. Thus, her calculations result in a gross underestimate of the mortality risk. Let’s get around that problem by looking at the risk that a child will die from measles before reaching five years of age, which is the time period during which 55% of measles mortalities occur (Orenstein et al. 2004).
There are currently roughly 177 million children under the age of five (census.gov/popclock), which gives us a mortality rate of 0.036% per year*. You might think that this means that there is a 0.6 in 100 chance of developing autism (using world-wide data), and a 0.036 in 100 chance of dying of measles before age five (using world-wide data), but that’s not actually fair either, because that estimate uses the death rates given our current vaccination status. If we remove vaccines, we jump to 1.14 million deaths per year, and our risk of death for children under five jumps to 0.35 in 100. At this point the mortality and autism rates are quite similar, but we aren’t even done yet, because Jaclyn specified at the beginning that she was talking about severe autism. I don’t know exactly what she counts as “severe,” but let’s assume that it is the top 50% of cases. Well then guess what, at that point, the autism risk for a child is 0.3 in 100 whereas the risk of measles death before the age of five is 0.35 in 100** (i.e., death from measles is more likely). Now, obviously the exact numbers will vary by country and what you count as “severe autism,” but the point is that when you actually do the math, in the absence of vaccines, the measles death rate would be very close (probably even greater) than the current rate of severe autism. Also note that this is just the probability of death prior to the age five, but 45% of measles deaths happen at later ages, so the overall mortality risk is actually much higher.***
In other words, if you want to agree with Jaclyn’s argument, you have to argue that death by measles is better than a life with severe autism, because if everyone stops vaccinating, then the risk of a child dying from measles will be roughly equal to the current risk of a child developing severe autism. So that (according to Jaclyn) is what you are choosing between: death or life with a disability. In reality, of course, you don’t have to choose because vaccines don’t cause autism. So your children can enjoy an exceptionally low risk of death by measles without it affecting their risk of developing autism.
*Note: I calculated the risk by taking the number of annual measles deaths (114,900; WHO 2016), multiplying by the proportion of mortalities that occur in children under five (0.55), dividing by the number of children on the planet (177 million), then multiplying by 100 to convert it into a percentage. The calculation for the death rate without vaccines was identical but it used 1.17 million deaths instead of 114,900.
**Note: the risk of death is actually much higher than I described here because I left out another really important factor. Namely, the autism risk is estimated per child (you only “get” autism once), but the measles deaths are per child per year, so there are four opportunities for death. I left this out of the calculations because the math is convoluted since most children only get measles once. As a result, the probabilities change each year, and the math was more intense than I felt like explaining here, but I thought it was worth at least mentioning that my estimate is actually a gross underestimate. (I’ve found that few people bother to read math-heavy posts, which is quite unfortunate).
***Note: I was too lazy to calculate the overall mortality risk, but if anyone feels like doing it, it is a cumulative probability. So you calculate the probability for each age class, then sum those. You have to do it this way because anyone who dies of measles in one age class is automatically eliminated from all subsequent age classes. In other words, if you try to do the math using a large age range (say 1–20) you won’t get reliable results, because the mortality risk for a 20 year-old is vastly different from the risk for a 1 year-old and, as a result, many 1 year-olds die and never make it to 20. The best way to think about this is that for each age bracket, you are calculating the mortality risk given that you survived to enter that age bracket. Thus, the mortality risk for children under five is quite high, but if you survive to age five, then the mortality risk before reaching age eight is much lower, and the overall mortality risk for a 0–7 year old is the sum of the risk from ages 0–4 and the risk from ages 5–7.
Conclusion/summary
In short, measles is in fact a very serious disease. It currently kills over well over 100,000 people annually, and it is estimated that without vaccines that number would be over one million. Further, you have to remember that the majority of measles deaths occur in children under five years old, so without vaccines, we would expect a minimum of 0.35 deaths per every 100 children age 1–4. That is not something that should be taken lightly or described as “benign.” Additionally, this entire post is based on a false dichotomy, because vaccines don’t cause autism. So you don’t have to choose between the risk of a measles death and the risk of autism, because getting vaccinated does not increase your chance of developing autism. In short, this post made one unscientific, misleading, and downright dishonest claim after another. The measles vaccine is extremely safe and effective, and you should not give in to the baseless fear-mongering.
Related Posts
Citations
- Antona et al. 2013. Measles elimination efforts and the 2008-2011 outbreak in France. Emerging Infections Diseases 19.
- Baxter et al. 2015. The epidemiology and global burden of autism spectrum disorders. Psychological Medicine 45:601–613.
- Bishop et al. 2008. Autism and diagnostic substitution: evidence from a study of adults with a history of developmental language disorder. Dev Med Child Neurol 50: 341–345.
- CDC 2004. Epidemiology of Measles—United States, 2001–2003. Morbidity and Mortality Weekly Report 53:713–716.
- CDC. 2011. Measles — United States, January–May 20, 2011. Morbidity and Mortality Weekly Report 60:666–668.
- CDC. 2015a. Measles (Rubeola): Complications of Measles. Accessed 20-Aug-16.
- CDC. 2015b. Vaccines & Immunizations: Measles–Q&A about Disease & Vaccine. Accessed 20-Aug-16.
- CDC. 2016a. Measles (Rubeola): For Healthcare Professionals. Accessed 21-Aug-16.
- CDC. 2016b. Autism Spectrum Disorder (ASD): Data & Statistics. Accessed 21-Aug-16.
- Christenson and Bottiger. 1994. Long-term follow-up study of rubella antibodies in naturally immune and vaccinated young adults. Vaccine 12:41–45.
- Clemens et al. 1988. Measles vaccination and childhood mortality in rural Bangladesh. American Journal of Epidemiology 128:1330–1339.
- Elsabbagh et al. 2012. Global prevalence of autism and other pervasive developmental disorders. Autism Research 5:160–179.
- Ewing. 2009. What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature? North American Journal of Medical Sciences 1:28–47.
- Gaurner et al. 2006. Mechanisms of disease: The hygiene hypothesis revisited. Nature Clinical Practice Gastroenterology and Hepatology 3:275–284.
- Hansen et al. 2015. Explaining the increase in the prevalence of autism spectrum disorders: the proportion attributable to changes in reporting practices. JAMA Pediatrics 169:56–62
- Jokinen et al. 2007. Cellular immunity to mumps virus in young adults 21 years after measles-mumps-rubella vaccination. Journal of Infectious Diseases 196:861–867.
- King et al. 1991. Clinical efficacy of measles vaccine during the 1990 measles epidemic. Paediatric Infectious Disease Journal 10:883–888.
- Knol et al. 2013. Large ongoing measles outbreak in a religious community in the Netherlands since May 2013. Eurosurveillance 18.
- Kockanek. 2011. Deaths: Preliminary Data for 2009. National Vital Statistics Reports 56.
- Mina et al. 2015. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. 6235:694–699.
- Murphy et al. 2010. Deaths: Final data for 2010. National Vital Statistics Reports 61.
- Rutter. 2005. Incidence of autism spectrum disorders: changes over time and their meaning. Acta Paediatr 94:2–15.
- Orenstein et al. 2004. The clinical significance of measles: a review. Journal of Infectious Diseases 189:S4–S16.
- Schmitz et al. 2011. Vaccination status and health in children and adolescents findings of the German health interview and examination survey for children and adolescents (KiGGS). Dtsch Arztebl Int 108:99–104.
- Sudfeld et al. 2010. Effectiveness of measles vaccination and vitamin A treatment. International Journal of Epidemiology 39:i48-i55.
- Taylor et al. 2014. Vaccines are not associated with autism: and evidence-based meta-analysis of case-control and cohort studies. Elsevier 32:3623-3629.
- Whitney et al. 2014. Benefits from immunization during the vaccines for children program era — United States, 1994–2013. Morbidity and Mortality Weekly Report 63:352–355.
- WHO. 2016. Measles. Accessed 20-Aug-16.