
One of the most common concerns that people have about vaccines is that they might cause (or exacerbate) autism. This idea is perpetuated by celebrities and innumerable websites, and it has become one of the cornerstone arguments of the anti-vaccine movement, but is there any truth to it? Perhaps unsurprisingly, both sides claim a superiority of evidence. Indeed, you can find numerous websites presenting lists of papers that they claim provide evidence that autism is caused by vaccines (such as Ginger Taylor’s list of “157 research papers supporting the vaccine/autism link“). Conversely, those who support vaccines also have lists of papers which they present as evidence that vaccines do not cause autism (for example, here, here, and here).
Which is correct? The internet is full of misinformation on this topic, so I want to cut through that crap and talk about the actual studies themselves rather than simply tossing lists around. In science, quality is often far more important than quantity, and you have to critically examine studies rather than blindly believing them (details here; here and here; examples here and here). So that is what I want to do in this post. I am going to walk you through both the anti-vaccine and pro-vaccine lists to see which position is actually supported by the evidence. I did this once before several years ago, but since then, the anti-vaccine lists have grown from 124 papers to 157 papers, and conversely, two new papers showing that vaccines do not cause autism have been published and are worth talking about. Therefore, I have updated the original post with the new papers on both sides, as well as re-writing some sections for improved clarity (you can read my original post here). You can also find excellent debunkings of the anti-vaccine lists at Stories from the trauma bay and I Speak of Dreams (here and here). I highly recommend reading those posts in addition to my own.
I have three key target audiences here. First, to any parents who are concerned about vaccines and are truly and sincerely looking for good information, I hope that this post will be a helpful tool for you and will dispel much of the nonsense on the internet. There are so many frightening stories and claims out there that I fully understand why you would be concerned. So I have done my best to thoroughly cover all of the evidence, and I hope that you will carefully consider it.
Second, for those who have already reviewed the evidence, but are tired of explaining it over and over again in debates, I hope that this post will provide a resource that will save you some time.
Third, for those who are not particularly interested in the autism/vaccine debate, I hope that this post will provide a nice worked example of how to critically analyze a large body of literature. There are, sadly, a lot of bad scientific publications out there, and it is important that you know how to sift through them and separate the high quality studies from the statistical noise.
Finally, to those who are already convinced that vaccines cause autism, although you are not my target audience, I do hope that you will read this, but I have one simple request to make of you. If you choose to continue reading, then I want you to seriously consider the possibility that you might be wrong. I want you to actually examine the evidence presented here rather than blindly ignoring it. If you aren’t willing to do that, then there is really no point in you continuing to read.
This post is necessarily long, so for your convenience, I have included a short summary section at the beginning which condenses the entire post into a few paragraphs. If you really want to understand this topic, however, I suggest that you skip past this section and read the detailed analyses of both the pro-vaccine and anti-vaccine literature. I have made a list of hyperlinks (below) that you can use to jump to any particular sections that interest you. You can also download an excel sheet with citations for Ginger’s list of anti-vaccine papers along with how I categorized them.
Following popular request, I have thrown together a crude .pdf of this post that you can download here.
Note: Throughout this study, I will refer to “pro-vaccine studies” and “anti-vaccine studies.” I am simply using those terms as an easy way to distinguish between studies that failed to find an association between vaccines and autism and studies that found an association (or are cited by ant-vaccers as evidence). Please do not misconstrue those terms or view them as implications that the research was biased or agenda driven.
- TL;DR
- The Autism/Vaccine Hypothesis
- Pro-Vaccine Studies
- Anti-Vaccers’ Lists of Papers
- Studies that weren’t about vaccines or weren’t about autism
- In vitro trials and animal studies
- Mercury and thimerosal studies
- Conference abstracts, case series opinions, other non-research papers
- Actual human studies on current vaccines and autism
- Reviews
- Conflicts of interest
- Overview of anti-vaccine papers
- Anecdotes, Court Cases, VAERS, etc.
- Annotated list of anti-vaccine papers (excel download)
About this update
When I wrote the original version of this post in 2016, Ginger’s infamous list of papers only included 124 entries. Since then, it grew to 130 then 157, so it seemed like it was time for an update. I was particularly curious to see what new evidence Ginger had found. In the original version of this post, I had pointed out that the evidence against the autism/vaccine hypothesis was extremely strong, with multiple high quality studies with tens of thousands of children, and even a meta-analysis with over one million children. Thus, for the anti-vaccine position to be viable, it would have to, at the very least, have equivalent evidence.
So what did Ginger come up with? Of the 34 studies she added, an astounding 23 papers weren’t about vaccines, one wasn’t about autism, four claimed to be about autism but were animal studies so their applicability is limited, one was an in vitro study (again, limited applicability), nine were non-systematic reviews or opinion pieces, and ten were on either forms of mercury that were never in vaccines or thimerosal, which hasn’t been in childhood vaccines for almost two decades (note: some studies were in multiple categories).
Only two of the new papers were on novel research that was conducted on humans and is relevant to the current vaccine schedule. However, both of those papers were published in a predatory journal (i.e., not a real science journal) and were based on an utterly terrible and completely invalid survey of homeschoolers. Indeed, one of those papers has already been retracted (more on those studies later).
Amusingly, she also added Khaled et al. (2016) to the list. This is entertaining because, while the study made no mention of vaccines, it did identify biomarkers which can be used at birth (i.e., before vaccines) to diagnose autism. In other words, it showed that autism is diagnosable before being vaccinated! Thus, this paper actually provides good evidence against Ginger’s claims (the irony is incredible).
It’s also worth briefly mentioning what Ginger didn’t do with the list. Namely, remove the irrelevant papers. As Liz Ditz, Doc Bastard, and I have been pointing out for years, many of the papers on the list simply have nothing to do with vaccines, autism, or both. Many of them literally don’t even mention vaccines, and the fact that Ginger refuses to remove them (and continues to add more irrelevant studies) shows a shocking level of either ignorance or intellectual dishonesty (most likely both).
To be fair, she did remove Inbar et al. (2016) from the list after that paper was withdrawn from publication, but that doesn’t change the fact the she refuses to critically examine most of the papers on her list and is clearly more interested in having a high paper count than in accurately reporting the state of the literature.
On the other side of things, several new studies have provided more evidence that vaccines don’t cause autism, and there are two that I have added to the discussion in this post. First, I’ve added Hviid et al. (2019), the massive Danish cohort study that has been in the press lately. Second, I added Goin-Kochel et al. (2016), which compared vaccination rates among children with different types of autism to see if there was an association specifically with regressive autism (as many anti-vaccers claim). Beyond the novel studies, I have also added Fombonne et al. (2006; a large time-series study in Canada) and Makela et al. (2002) which looked at the timing of autism diagnosis following vaccination.
Additionally, I have removed Price et al. (2010) and Verstraeten et al. (2003) from my main count of large studies, and I have re-framed how I discussed them. I did this because they specifically examined thimerosal containing vaccines, so removing them from the main count seemed more consistent with how I treated the anti-vaccine studies on thimerosal, and, unlike Ginger, I really do strive for intellectual honesty. I apologize if my previous treatment of those papers caused any confusion. It was not my intention to mislead anyone.
Finally, I have rewritten several parts of this, expanding some sections, shortening others, and even adding some new sections. So this is a fairly major overhaul of the previous version.
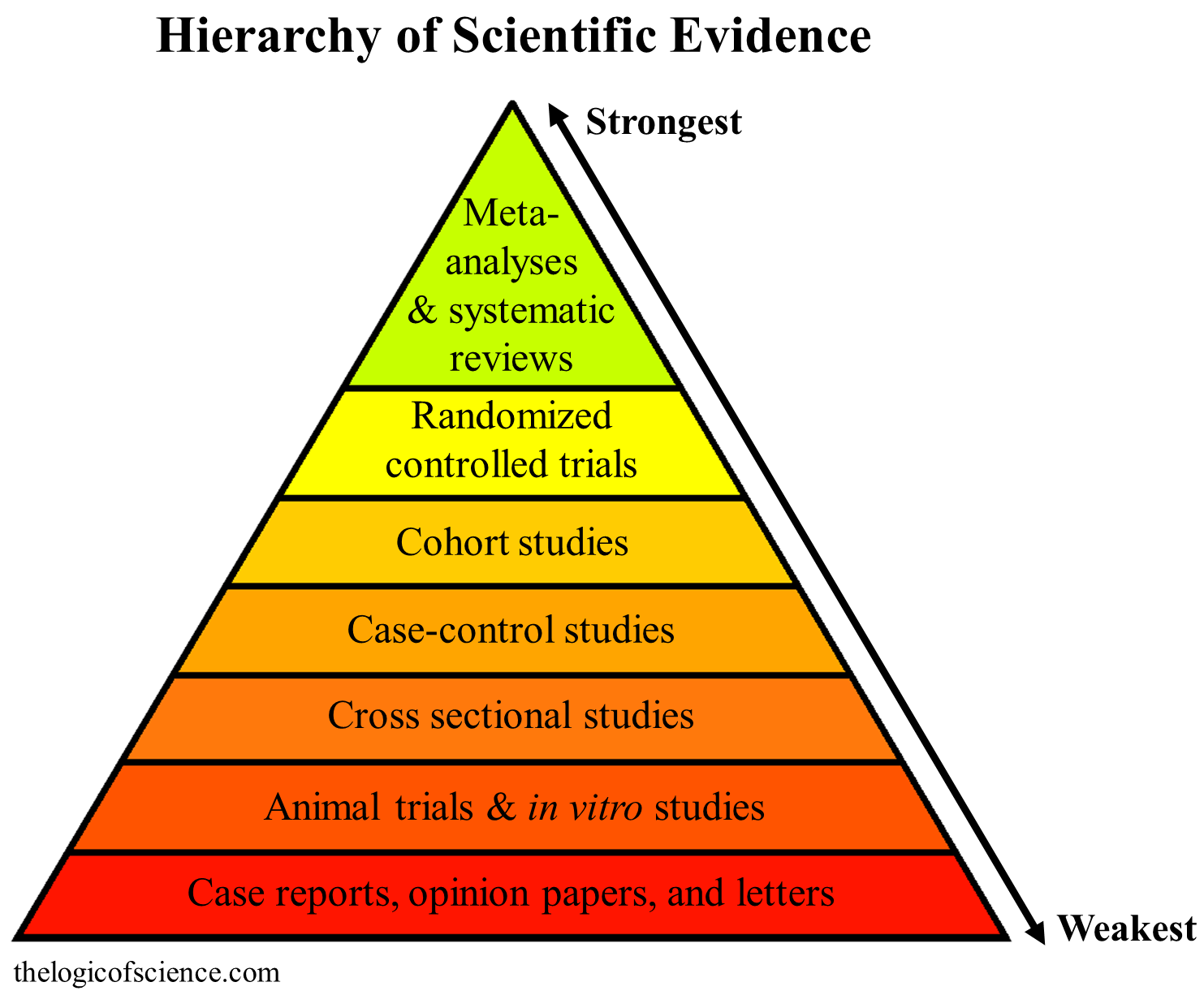
Not all study designs are equal (details here)
TL;DR
I want to start with the pro-vaccine lists (for example, here and here). These lists boast well over 100 studies, but many of those papers are admittedly small, used relatively weak designs, are non-systematic reviews, or aren’t relevant for the current vaccine schedule. So I am just going to focus on the really high quality evidence, because there is a lot of it.
Several studies have either looked for general correlations between autism rates and vaccines (Fombonne et al. 2006; Dales et al. 2001) or have looked for changes in autism rates following either the introduction (Taylor et al. 1999; Chen et al. 2004) or removal (Honda et al. 2005) of the MMR vaccine. None of these studies found a significant relationship.
Other studies have used a more robust design known as a case-control analysis (Destefano et al. 2004 [642 people with autism; 1824 people without autism]; Smeeth et al. 2004 [991 with*; 4469 without]; DeStefano et al. 2013 [256 with; 752 without]; Uno et al. 2015 [189 with, 224 without]). Case-controlled studies start with two groups (one with and one without the effect of interest) then work backwards to test a potential cause. This makes them a very powerful design for detecting associations with relatively rare events (such as autism*), yet none of these studies found those associations.
*Note: Although autism is common, it is still rare enough that you need very large sample sizes for most studies before you can detect significant changes. Case-control studies solve that problem by starting with a group that already has autism, then working backwards.
Next, we have cohort studies that compared autism rates between children who did and did not receive the vaccine being studied. This is one of the most powerful experimental designs, and these studies were particularly large (Hviid et al. 2019 [657,461 children]; Madsen et al. 2002 [440,654 children]; Anders et al. 2004 [109,863 children]; and Jain et al. 2015 [95,727 children]). Take another look at those sample sizes, they are enormous (far larger than any of the anti-vaccine studies), but once again, they did not find any significant differences between vaccinated and unvaccinated children.
Further, there is a meta-analysis with over 1.2 million children (Taylor et al. 2014) which also failed to find evidence of vaccines causing autism. Meta-analyses are the most powerful type of paper because they combine the results from multiple studies, thus greatly reducing the odds of a false result. Further, the larger the sample size, the more powerful the study. So this meta-analysis is the most powerful method available, and it used an incredibly large sample size, which makes it an extremely robust and convincing study.
Additionally, there are also studies that looked at whether vaccines can specifically cause regressive autism, and they also failed to find a significant effect of vaccines (Richler et al. 2006; Uchiyama et al. 2007; Goin-Kochel et al. 2016).
On the anti-vaccine side, I went through their lists of papers (here, here, and here; 160 papers total), and 33 of them weren’t actually about autism, 82 (over half) weren’t about vaccines, 41 were animal trials or in vitro studies (which are weak designs that have limited applicability to humans, especially for something like autism), 60 were on either a form of mercury that has never been in vaccines or thimerosal (which hasn’t been in childhood vaccines for almost two decades), 9 were case reports/conference abstracts/opinion papers/some other non-research paper, and 37 were non-systematic reviews (only 8 of which were relevant to the topic at hand; some papers were in multiple categories).
Only 14 of the papers were actually studies on humans that are relevant to autism and the current vaccine schedule, but none of those studies were large, all of them were association studies (i.e., they could not show causation, because correlation does not equal causation), and most of them were seriously flawed. Additionally, many of them relied on the idea that autism rates are increasing, but there is a substantial amount of evidence that the increase is largely (if not entirely) due to changes in how autism is diagnosed rather than an actual increase in the number of people with autism (Rutter 2005; Taylor 2006; Bishop et al. 2008; Baxter et al. 2015; Hansen et al. 2015). Finally (and most amusingly), one of those 14 studies was actually a pro-vaccine study that directly contradicted the results of two of the other studies.
Thus, when you consider all of the evidence, it is completely fair to say that the scientific evidence overwhelmingly supports that conclusion that vaccines do not cause autism, and there is no reliable evidence to the contrary. To be clear, that’s not just the opinion of a blogger. Rather, at least seven systematic reviews have looked at the literature and come to the exact same conclusion (Jefferson et al. 2003; Klein and Diehl. 2004; Parker er al. 2004; Hurley et al. 2010; Stratton et al. (eds). 2011; Demicheli et al. 2012; Margaret et al. 2014).
To be fair, the anti-vaccers also have reviews, but none of their reviews were systematic (Rimland and McGinnis. 2002; Singh. 2009; Ratajczak 2011; Sienkiewicx et al. 2012;Shaw and Tomljenovic. 2013b; Shaw et al. 2014a; Morris et al. 2017a; Lyons-Weiler 2018). This is important because systematic reviews use pre-defined search terms and criteria to find papers. Thus they include all of the relevant papers, regardless of whether they were pro or anti-vaccine. In contrast, non-systematic reviews include whatever papers the authors felt like including. As a result, it should not surprise you to learn that the anti-vaccine reviews ignored the large meta-analysis, cohort studies, etc. and instead focused on the small studies. In other words, they painted an inaccurate and deceptive picture that did not represent the actual state of knowledge. Further, none of the papers cited in those reviews actually presented concrete evidence of vaccines causing autism. Rather, the reviews constructed hypotheses about how vaccines could in concept cause autism. That would be fine if it wasn’t for the fact that those hypotheses have been tested and discredited via the case-controlled studies, cohort studies, etc. In other words, if the hypotheses were true, those studies should have found evidence of vaccines causing autism, but they didn’t. Therefore, we must reject the hypotheses.
In short, the idea that vaccines cause autism has been extremely thoroughly tested by numerous scientists working for different universities and organizations from around the world. It has been tested via multiple different methods and populations, and it has been addressed from multiple angles (e.g., different vaccines, different vaccine components, age at vaccination, number of antigens, number of doses, etc.), and the result is exceptionally clear: vaccines do not cause autism. There are no large, properly controlled, epidemiological studies that disagree with that result. For more details about both the pro and anti-vaccine studies, please read the rest of this post.
Note: very few of the pro-vaccine papers had conflicts of interest (i.e., they were not funded by pharmaceutical companies), and conflicts of interest were present in many of the anti-vaccine papers. More details are provided in the rest of this post.
Jump back to the top
The Autism/Vaccine Hypothesis
Science is all about making hypotheses and testing whether or not their predictions come true. Therefore, it is always a good idea to establish exactly what you are asking before you look at the literature. In this case, the question is whether or not vaccines cause autism, but that needs to be nuanced a bit. According to the CDC, about 1 in 59 children in the US have autism, with other developed countries reporting varying, but largely comparable levels (Elsabbagh et al. 2012). Those numbers have gone up over time, which has led anti-vaccers to refer to the situation as an “autism epidemic,” and they often make dire predictions like, by 2022 autism rates will be 1 in 9. I’m not going to take the time to explain why that math is absurd, but I will point out that there is a large body of evidence showing that most, if not all, of the increase in autism rates is due to changes in how autism is diagnosed (Rutter 2005; Taylor 2006; Bishop et al. 2008; Baxter et al. 2015; Hansen et al. 2015). In other words, autism rates are higher now than they were in 1990 because people who would not have been considered autistic in 1990 are considered autistic today (Dr. Novella wrote a good post on this several years ago that includes some additional sources).
The point is that we have two different hypotheses that make different predictions. If vaccines are actually causing an autism epidemic, then when we compare vaccinated and unvaccinated children, we should find that autism rates are much lower among the unvaccinated children. If vaccines don’t cause autism, however, then the rates should be the same. Importantly, the larger our sample sizes, the more power that we will have to detect significant differences. In other words, even if vaccines are only responsible for a very small portion of autism cases (rather than an epidemic), we could still detect that with a large enough sample size. Now, with that in mind, let’s see what we find in the literature.
Studies that failed to find evidence of vaccines causing autism
I want to start with the pro-vaccine studies, and there are quite a few of them. Indeed, you can find several lists on the internet that boast over 100 studies demonstrating that vaccines do not cause autism (for example, here and here). I am, however, a bit cautious about lists like this. They can be quite useful, and I have linked to them multiple times on this blog, but a quick examination of these lists will reveal that they do actually contain quite a few low quality studies with weak designs or tiny sample sizes, opinion papers, etc. So I am not going to talk about all of the studies in these lists. Rather, I have painstakingly gone through them to eliminate all of the studies with really weak designs (like animal studies), tiny sample sizes, questionable statistics, etc. This type of filtering is a really good idea when you are examining a topic because it weeds out the statistical noise and leaves you with the reliable studies (importantly, however, you need to have a good understanding of experimental design, statistics, etc. before you can do this properly).
My filtering left me with six correlation/time-series studies, five case-control studies, four cohort studies, one meta-analysis, and seven systematic reviews that examined the hypothesis that vaccines cause autism. These studies provide the backbone of evidence, but there are many other studies which build on that backbone, some of which I will discuss. Additionally, many of the smaller studies that I left out are uncompelling on their own, but their cumulative effect is convincing (see the section on systematic reviews).
Jump back to the top
Correlation/time-series
Several different designs were used for these studies. One of them simply looked for correlations between vaccine coverage and autism rates (Dales et al. 2001). If vaccines cause autism, we would, of course, expect there to be higher autism rates when vaccine coverage is higher; however, this study failed to find that trend (i.e., vaccination rates and autism rates were not correlated). Similarly, Fombonne et al. (2006), used data on 27,749 children in Montreal, Canada from 1987 to 1998 to look at pervasive developmental disorders (including autism) over time and how they associated with MMR vaccine coverage, MMR dose (one vs two), and thimerosal exposure. There were no associations in any comparison, and total developmental disorders were actually highest when MMR coverage was the lowest
Another pair of studies specifically looked for changes in autism rates when the MMR vaccine was introduced to the UK (Taylor et al. 1999; Chen et al. 2004). The MMR vaccine is a favorite target of anti-vaccers, and if it actually causes autism, then we should see a spike in autism rates immediately following the introduction of that vaccine into a population, but neither study detected a significant change.
Another study, (Honda et al. 2005) took the opposite approach. In 1993, Japan abruptly stopped using the MMR vaccine, so Honda et al. (2005) examined the autism rates across the entire city of Yokohama (roughly 300,000 people) from 1988-1996. This study provides a nice balance to Taylor et al. (1999) and Chen et al. (2004), because just as you would expect autism rates to spike following the introduction of MMR (if MMR caused autism), you would also expect the rates to drop after the vaccine is removed. Just like the previous studies, however, Honda et al. (2005) failed to find any evidence of the vaccine causing autism (i.e., autism rates did not drop when the MMR vaccine was removed).
It’s worth pointing out that these types of studies cannot establish causation, because they only show correlation, and correlation does not automatically equal causation. The fact that two things occur together does not mean or even suggest that they are causally related. Nevertheless, a lack of correlation does suggest a lack of causation. In other words, if X causes Y, then X will be correlated with Y. So if X and Y are not correlated, that also suggests that there is no causal relationship between them.
Finally, Makela et al. (2002) took a very different approach and took a group of 535,544 who received the MMR vaccine and followed them to see if and when they developed autism. The idea was that if the anecdotes about vaccines quickly leading to autism were correct, then autism diagnoses should have clustered shortly after receiving the vaccine. As you might have guessed, they did not cluster (I talked about why we expect some cases to follow vaccines just by chance here).
Note: this type of time-series design was not included in the original image on the hierarchy of evidence that I have been including throughout this post, but these studies would usually rank about the same as a cross sectional study.
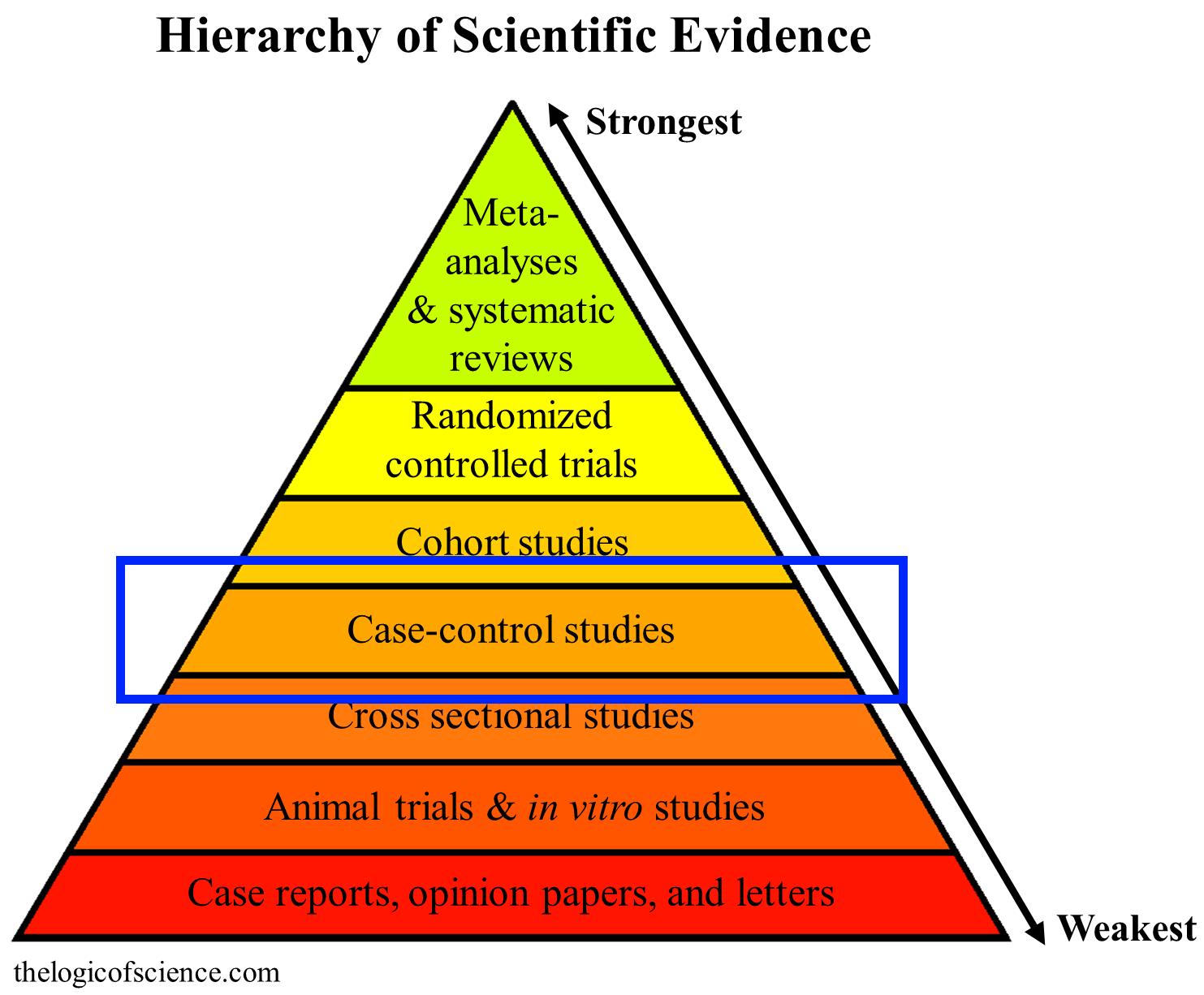
Case-control studies can’t establishes causation, but they are one of the best designs for looking for associations with rare relatively rare outcomes (e.g., autism). Details here.
Case-control studies
Case control studies are another type of correlation study, but rather than simply looking for correlations in a population, they take two groups that are similar except for an outcome (e.g., autism). They then work backwards to test for a potential cause of that outcome (e.g., you compare a group with and without autism to see if they differ in their vaccination rates). This design can only show association rather than causation, but it is very a very powerful way of at looking at relatively rare outcomes, and it allows you to get very robust results out of relatively small sample sizes (compared to other designs), making it an excellent method for looking for associations between vaccines and autism.
I found four reasonably large case-control studies that examined autism rates and are relevant to the current vaccine schedule (Destefano et al. 2004 [642 people with autism; 1824 people without autism]; Smeeth et al. 2004 [991 with*; 4469 without]; DeStefano et al. 2013 [256 with; 752 without]; Uno et al. 2015 [189 with, 224 without]). None of these studies found evidence that vaccination was associated with the development of autism.
Additionally, although all of these studies addressed the question of vaccines and autism, several of them were focused on a particular facet of the question or examined multiple sub-questions. For example, Destefano et al. (2004), Smeeth et al. (2004), and Uno et al. (2015) looked specifically at the MMR vaccine, whereas DeStefano et al. (2013) took an entirely different approach and looked at antigen exposure. This is really important because one of the most common tropes of the anti-vaccine argument is the, “too many too soon” argument, which argues that the antigens in vaccines will overwhelm a child’s immune system and lead to problems like autism. This study directly addressed that concern.
Several of these studies also looked at whether or not the age at vaccination was important for the development of autism, thus addressing the argument that vaccines should be delayed (Destefano et al. 2004; Smeeth et al. 2004; Uno et al. 2015). In all fairness, Destefano et al. (2004) did find slightly higher vaccination rates among the autistic children for their 36 month age-group (93.4% vs 90.6%), but there were no differences at 18 or 24 months, and in the case of the 36 month-olds, many of them had started to show signs of autism before receiving the vaccine, so the vaccine was clearly not at fault.
Another study (Goin-Kochel et al. 2016) took a different approach. Many anti-vaccers have shifted the goal posts from saying that vaccines cause autism to saying that vaccines specifically cause regressive autism. They use this to try to dismiss many of the existing studies by arguing that they looked at autism generally, rather than specifically looking at regressive autism. This argument is a logically invalid ad hoc fallacy (i.e., it is an assumption being made to patch a hole in an argument), but Goin-Kochel et al. (2016) tested it anyway. They took a large group of people with autism, grouped them by type of autism, then compared vaccination rates among the groups. If vaccines specifically cause regressive autism (as anti-vaccers suggest), then the vaccination rates should have been higher in the regressive autism group, but the study found no consistent significant differences among groups. This conclusion has also been supported by other studies (Richler et al. 2006; Uchiyama et al. 2007).
Finally, I want to briefly mention Price et al. (2010). This case control study (256 with autism; 752 without) looked specifically at thimerosal exposure from vaccines and immunoglobulin injections. It also found no associations. I have not included it in my main count of studies, however, because thimerosal was removed from childhood vaccines nearly two decades ago (the exact date varies by country, but its usually 1999-2001; certain formualtions of the flu vaccine still have thimerosal, and in Austrlaia, the Hep B vaccine still has it). Thus, thimerosal studies are no longer relevant for the current vaccine schedule.
*Note: Smeeth et al. (2004) also did a larger analysis of 1294 people diagnosed with “pervasive developmental disorders” which included those diagnosed with autism and those diagnosed with other developmental disorders, and that analysis also failed to find a significant effect of vaccines.

Cohort studies can be very powerful (especially with large sample sizes) and can actually show causation (details here).
Cohort studies
Next, we have the cohort studies. These work in the opposite direction from case-controlled studies. They start with a group of people (cohort) that are similar except for their exposure to some potential cause (e.g., vaccines). Then, the researchers track these individuals to see if they eventually differ in some outcome (e.g., autism). In other words, if vaccines cause autism, then you expect the members of the cohort that received vaccines to develop autism significantly more frequently than the members of the cohort that were unvaccinated.
I found many small cohort studies, but only four of them were large enough to be worth talking about in the context of the modern vaccine schedule (IMO). Those four studies were, however, extremely large and provide very convincing evidence that vaccines do not cause autism. Anders et al. (2004) used 109,863 children to study the DTP/DT vaccine, Hviid et al. 2019, Madsen et al. (2002) and Jain et al. (2015) used 657,461 children, 440,654 children, and 95,727 children (respectively) to examine the MMR vaccine. Really think about those numbers for a minute. Those sample sizes are extraordinary and gave the researchers tremendous power to detect significant trends, yet none were found.
As with the case-control studies, several of studies also examined additional aspects of the topic. For example, Madsen et al. (2002) also examined the effects of age at vaccination, and did not find a significant effect. Hviid et al. (2019) examined several other factors, such as the timing of an autism diagnosis following a vaccination (like Makela et al. 2002, which I discussed earlier). They also tried grouping children by previous vaccination history (i.e., vaccines other than the MMR) to see if the cumulative effect of lots of vaccines plus the MMR would make a difference, and the results were still negative. This is a very useful result because anti-vaccers often criticize these studies for only looking at a single vaccine, but this study included vaccine history in its analyses and still failed to find evidence of vaccines causing autism.
Perhaps most importantly, Jain et al. (2015) also looked specifically at a subset of 1,929 children who had a sibling with autism. This is a brilliant design because we know that autism has a genetic component. Even most anti-vaccers agree with that, they just argue that the genes make you more susceptible to the effects of vaccines. If that was the case, however, then it should be much easier to detect vaccine-associated autism in children who have a sibling with autism. In other words, infants who have an older sibling with autism have a higher risk of developing autism than infants whose siblings do not have autism (i.e., if your sibling has autism, then it is likely that the genes that predispose you to it are in your family). This means that by examining siblings, you are looking at a “high risk” group, thus maximizing your statistical power. Even with this design, however, they failed to find any significant effects of vaccines.
Hviid et al. (2019) also incorporated this sibling design and failed to find a significant effect, but their sample size for this subset test (37 children) was admittedly too small to be compelling. However, they also used other factors that are thought to increase a child’s risk of autism to create subgroups of children with a moderate risk (2312 children) or high risk (1048 children), then the looked for associations between autism and vaccination in those subgroups. Once again, there were no significant effects of vaccines. This lack of association in high risk groups is very strong evidence that vaccines are not a cause of autism.
Finally, I want to briefly talk about Hviid et al. (2003) and and Verstraeten et al. (2003). I did not include those studies in my main list because unlike all of the other studies that I have been talking about, they looked specifically at thimerosal (which is no longer in childhood vaccines). Verstraeten et al. (2003) used a cohort of 124,170 to look at cumulative thimerosal exposure, while Hviid et al. (2003) use a cohort of 446,695 children to compare vaccines with thimerosal to vaccines without thimersoal. Discussions of thimerosal are fairly pointless since it was removed from childhood vaccines almost two decades ago. Nevertheless, I want to make a few brief points.
First, anti-vaccers often accuse thimerosal of being the causative agent of autism (despite its absence from the current schedule), and these massive studies provide powerful evidence against that hypothesis. Second, Hviid et al. (2003) also looked at dose effects and failed to find any evidence of increasing autism with increasing vaccine dose. This is significant, because even if there was something in vaccines other than thimerosal that was causing autism, you would still expect that to show up in this study. Finally, the inclusion of dose once again provides evidence against the “too many too soon” argument.
Jump back to the top
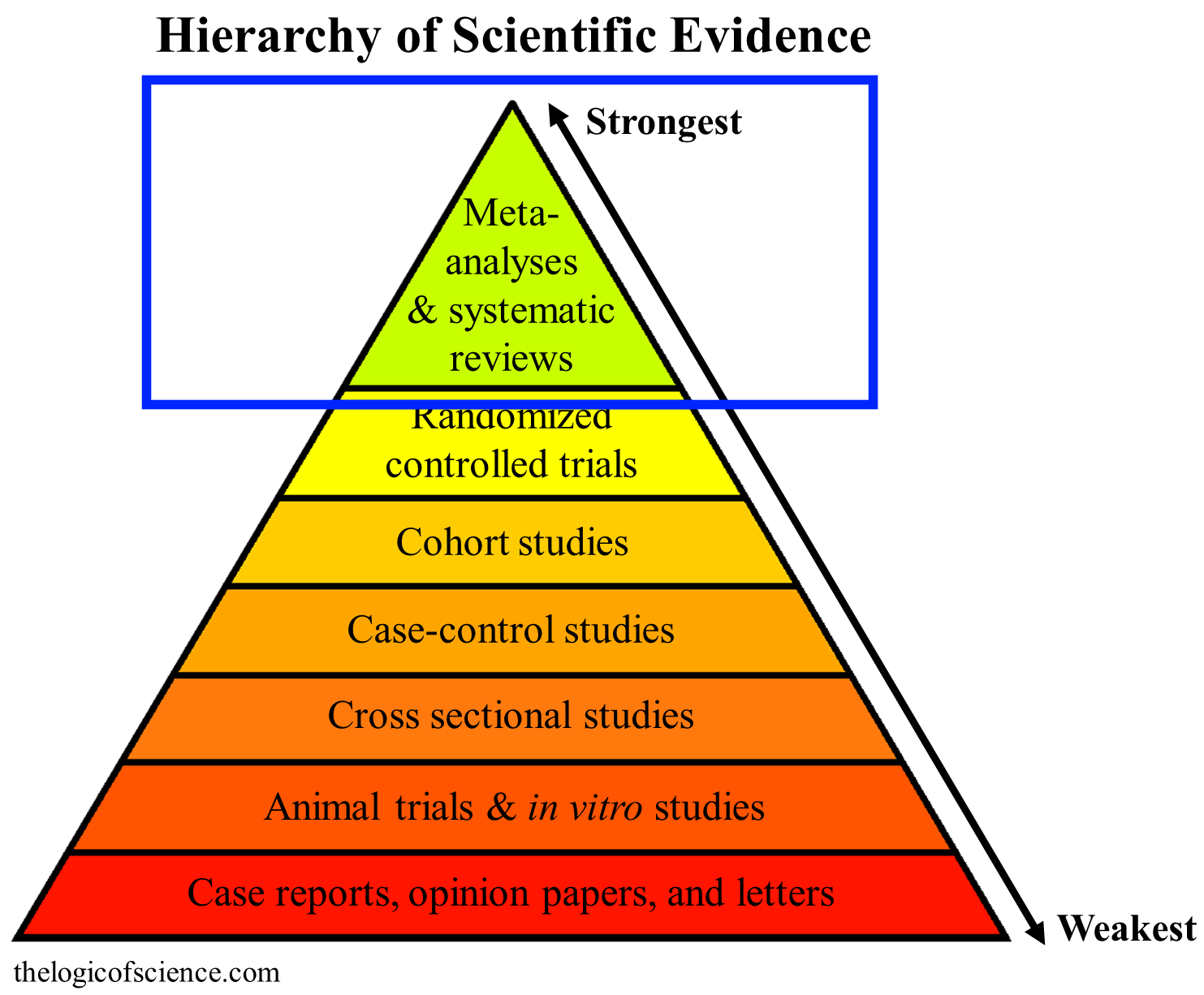
Systematic reviews and meta-analysis are the highest category of evidence because they combine the results of multiple studies, which makes them less prone to false conclusions (details here).
Systematic reviews
At the start of this section, I want to distinguish between a systematic review and a general or non-systematic review. A systematic review looks for papers using a predefined set of search terms and databases. For example, you might search PubMed and Web of Science for papers containing both the terms “vaccine” and “autism.” Then, you take that list of papers and filter by some other pre-defined criteria. For example, you might be interested only in studies that were case-controlled, cohort, or randomized controlled trials. Then, you write the review on the papers that are left.
Setting up reviews this way with pre-defined search terms and inclusion criteria is a really powerful way to comb through the scientific literature because it avoids bias. If a study meets your criteria, then it gets included regardless of what its conclusions were. Thus, you get a fair and accurate representation of the literature. To be clear, you can still bias these if you use absurd search terms (like, “vaccines do not cause autism,” for example), so you should always check systematic reviews to see what their inclusion criteria were.
In contrast, non-systematic reviews use any papers that the authors thought should be included. These reviews can still be quite good, but they also can be very problematic because the authors’ biases can have major influences over the papers that get included. If you are anti-vaccine, for example, you can write a “review” that only includes anti-vaccine papers, and ignores all of the pro-vaccine papers, thus creating the illusion that there is an overwhelming amount of evidence against vaccines (we’ll encounter some of those later in this post). The inverse is, of course, also true. A pro-vaccine scientist can bias a review just as easily as an anti-vaccine scientist. This is why systematic reviews are much better than regular reviews, and when you have multiple systematic reviews that all agree with each other, you can be fairly confident that the literature is pointing in a consistent direction.
In the case of autism, that direction is most decidedly away from a link between autism and vaccines. I found seven different systematic reviews of the topic, and they all said the same thing: the evidence does not support an association between vaccines and autism (Jefferson et al. 2003; Klein and Diehl. 2004; Parker er al. 2004; Hurley et al. 2010; Stratton et al. (eds). 2011; Demicheli et al. 2012; Margaret et al. 2014). I also found several non-systematic reviews that concluded that vaccines don’t cause autism, but I decided not to include them for the reasons explained above.
On a side note, Demicheli et al. (2012; a lengthy and thorough Cochran review ) also found that, “Exposure to the MMR vaccine was unlikely to be associated with autism, asthma, leukaemia, hay fever, type 1 diabetes, gait disturbance, Crohn’s disease, demyelinating diseases, bacterial or viral infections.”
Jump back to the top
Meta-analysis
Finally, we have a meta-analysis. Meta-analyses are the single most powerful tool available to scientists, because they actually pool the results of multiple studies, and run statistics on that pooled data set. This provides much larger sample sizes than you could normally achieve, and it largely overcomes the fact that sometimes a study reaches the wrong conclusion just by chance (i.e., the odds of the pooled data from multiple studies producing an erroneous conclusion is much, much lower than the odds of a single study being wrong). As a result, these studies are considered to be the highest level of evidence.
There is only one large meta-analysis for vaccines and autism, but it’s a big one (Taylor et al. 2014). It had a sample size of over 1.2 million children, which is an extraordinarily large sample size that provides tremendous statistical power. Nevertheless, this study did not find any associations between autism and vaccines (or thimerosal or mercury for that matter). That is as conclusive of an answer as you could ever hope to have.
Jump back to the top
Randomized-controlled trials
There are no large randomized controlled trials on vaccines and autism, and there are two very good reasons for that. First, autism is rare enough that you would need an absurd sample size to have a reasonable chance of detecting a significant effect. So they aren’t practical (case-controlled and cohort studies are more well-suited to the question at hand). Second, the benefits of vaccines have been established beyond any shadow of a doubt, so it would be unethical to deliberately give people placebos rather than vaccines.
The lack of randomized controlled trials is not a problem, however. Randomized controlled trials are the most powerful experimental tool for establishing causation, but the other methods are perfectly capable of showing a lack of causation. For example, case-controlled trials can only show correlation, not causation, but since a lack of correlation also means a lack of causation, they can be very powerful tools for showing that two things are not causally related. So if you were arguing that vaccines cause autism, then a lack of randomized controlled trials would be potentially problematic (depending on the strength of the other studies, especially the cohort studies), but the lack of randomized controlled trials is really irrelevant for this negative result.
Jump back to the top
Regressive autism, multiple doses, age at vaccination and other sub-hypotheses
At this point, I want to pause for a minute to deal with some common criticisms and point out just how broad the literature is. Anti-vaccers are masters at shifting goal posts, and, as a result, scientists are forced to study a constantly shifting hypothesis. It’s like fighting the hydra. Every time we falsify one hypotheses, anti-vaccers invent two more, rather than simply accepting the results.
For example, a common criticism I hear is that many of the studies I’ve been talking about focused specifically on the MMR vaccine. However, this criticism ignores the fact that scientists have focused on the MMR vaccine because that is the vaccine that anti-vaccers singled out as the cause of autism! In other words, scientists tested anti-vaccers’ hypothesis, but anti-vaccers didn’t like the answer to those tests, so they changed the hypothesis, then accused scientists of not addressing the “real issue” (also, there have been large studies that looked at vaccines other than the MMR, e.g., Anders et al. (2004)). I’ve tried to point out some of these hypotheses as I’ve gone through the studies, but to make it easy, here is a non-exhaustive list of sub-hypotheses that scientists have looked and falsified (specifically within the overarching hypothesis that vaccines cause autism):
- The hypothesis that vaccines cause regressive autism (Richler et al. 2006; Uchiyama et al. 2007; Goin-Kochel et al. 2016)
- The hypothesis that vaccines only cause autism in high risk/sensitive children (Hviid et al. 2019; Jain et al. 2015)
- The hypothesis that the age at vaccination matters (i.e., the “too many too soon” argument”; Uno et al. 2015; Destefano et al. 2004; Smeeth et al. 2004; Madsen et al. 2002)
- The hypothesis that it is the total antigen count that matters (another version of the “too many too soon” argument; DeStefano et al. 2013)
- The hypothesis that too many doses cause autism (yet another version of the “too many too soon” argument; Fombonne et al. 2006; Hviid et al. 2003)
- The hypothesis that it is the cumulative effect of vaccines that matters (yet another version of the “too many too soon” argument; Hviid et al. 2019)
- The hypothesis that its thimerosal (Hviid et al. 2019; Taylor et al. 2014; Price et al. 2010; Hviid et al. 2003; Verstraeten et al. 2003)
I also want to point out that some of the more popular hypotheses that have not been directly addressed have actually been discredited by the existing literature. For example, the hypothesis that aluminum in vaccines is the culprit (which became popular once it was clear that thimerosal wasn’t the problem) should have caused an increase in autism among vaccinated children in studies that looked at things like dose and age at vaccination. The fact that those studies were negative discredits the hypothesis.
Conflicts of interest
At this point, you may be thinking, “but all of those studies were conducted/paid for by pharmaceutical companies, so they can’t be trusted!” I anticipated that argument and checked for conflicts of interest as I went through these papers. I only found eight, and only two of them were serious enough to be at all concerning.
First, for two of the case-controlled studies (Smeeth et al. 2004; Price et al. 2010), some of the authors had previously received funding from pharmaceutical companies for other projects. In other words, these two studies were not funded by pharmaceutical companies, and the authors don’t work for those companies, but the companies had funded some other projects that were conducted by some of the researchers. That’s hardly damning evidence of corruption.
Two of the other conflicts surrounded Dr. Jefferson. In 1999, he worked as “an ad hoc consultant for a legal team advising MMR manufacturers.” This was acknowledged in his review (Jefferson et al. 2003) and in Demicheli et al. (2012). Jefferson was not an author on the final paper for Demicheli et al. (2012), but the paper stated, “The review authors wish to acknowledge Tom Jefferson and Deirdre Price as previous author.” In other words, he was involved at some stage, but not with the final product. Once again, showing that one of the researchers involved used to be a consultant for a legal team hardly indicates that all of his research has been corrupted. Similarly, Dr Fombonne, who wrote Fombonne et al. (2006), has given advice to pharmaceutical companies, has been on government panels, and has been an expert witness in vaccine lawsuits, but has never received research funding from pharmaceutical companies.
Another one of the conflicts also comes from a review. Hurley et al. 2010 stated, “All authors are employed by MED Communications, Inc., which provides medical and drug information services to multiple pharmaceutical firms, including several manufacturers of various vaccines.” So they were employed by a company that provides info to vaccine manufacturers, but they were not employed by the vaccine manufactures themselves. Again, that’s not really concerning.
Finally, the two potentially serious conflicts are from the funding for Hviid et al. (2019) and Makela et al. (2002). Hviid et al. was partially funded by the Novo Nordisk Foundation. This foundation funds a large number of research projects, but it also owns several pharmaceutical companies (the rest of the funding came from the Danish Ministry of Health). However, as the paper says, “The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.” The conflict in Makela et al. was more direct. It was partially funded by Merck.
To be clear, conflicts of interest do not automatically negate papers. Conflicts of interest should make you scrutinize a paper more closely, not automatically reject it.
Nevertheless, let’s say that you did want to completely reject those eight studies. That would still leave you with four correlation/time-series studies, three case-control studies, three cohort studies, four systematic reviews, and one massive meta-analysis, all of which provide compelling evidence that vaccines are safe and, as far as I can tell, did not have conflicts of interest. They were funded by numerous different agencies, and the researchers worked for various universities, hospitals, and government agencies from all over the world (you can find more details about the funding for some of these studies here).
I’ll also briefly add here that I have never received any money from pharmaceutical companies, and I do not get paid to write this blog. In fact, it costs me money, because I am using a free wordpress account (so I don’t make money from adds, nor do I have any control over them), and I pay an annual fee for a domain name.
Jump back to the top
Sample size and statistical power
Before I leave this section, I want to make a very important point about that nature of negative results in science. Technically speaking, it is not actually possible to demonstrate that vaccines don’t cause autism, but it is possible to demonstrate that if they cause it, they do so at a very low rate. In other words, if you have a sample size of 100 people, you haven’t tested the possibility that vaccines cause it at a rate of 1 in 1000, and if you have 1000 people, you haven’t tested the possibility that vaccines cause it at a rate of 1 in 10,000, etc. (note: those numbers are not precise). So no matter how large your sample size is, it is always possible that the effect is just smaller than what you were able to detect.
Now, when we apply that to vaccines and autism, what we see is that if vaccines do cause autism they do so at an absurdly low rate. Scientists have conducted a meta-analysis with over 1.2 million children, several cohort studies with close to or over 100,000 children, several large case-controlled studies, and studies that looked specifically at children who were at a high risk of developing autism. This means that we could have detected even a very a very low rate of vaccines causing autism. It’s a bit difficult to calculate exactly what that rate is, but even a rate of about 1 in 10,000 would likely show up in the larger studies.
Remember, however, that the claim being made by anti-vaccers is that vaccines are causing an “autism epidemic,” and that claim is clearly false. Even if vaccines were only responsible for 5% of autism cases, that would be a rate of less than 1 in 1,300 people, which is well within the range that these studies had the power to detect. Further, even if vaccines only caused 1% of autism cases, that would be a rate of 1 in 6,800 people, which is still low enough that we should have detected it.
My point here is that these studies had an extraordinary power to detect even very tiny effects of vaccines, yet they failed to find any evidence of vaccines causing autism. This means, that if vaccines do cause autism, they do so at an incredibly low rate that shouldn’t be concerning (remember, every decision has risks, including the decision not to vaccinate).
To be 100% clear here. I am not in any way shape or form suggesting that vaccines actually do cause autism at a very low rate. There is utterly no evidence to think that they do (thus assuming that they do is an argument from ignorance fallacy). Rather, I am bringing this up because I am trying my best to give a fair and honest representation of the current state of our knowledge, and it is not technically correct to say that we have demonstrated that vaccines don’t cause autism, because what we have actually done is demonstrate that it is very unlikely that vaccines cause autism at a meaningful rate, or, to put it another way, if they cause autism, they do so at an extremely low rate, which still means that anti-vaccers’ claims are false.
Jump back to the top
Anti-Vaccers’ Lists of Papers
Introduction to anti-vaccers’ papers
Before I go into the lists of papers that, according to the anti-vaccers, demonstrate that vaccines cause autism, I want to specify exactly what we would need to find in order for anti-vaccers’ claims to be legitimate. Remember, sample size and experimental design are extremely important in determine the quality of a study. Therefore, given that we have very large case-controlled and cohort studies, as well as a meta-analysis with over 1.2 million children, all of which say that vaccines don’t cause autism, for the claim that vaccines do cause autism to be plausible, we would need multiple studies of similar size and power. That’s how science works. You don’t get to trump a massive meta-analysis with a tiny association study. So with that in mind, let’s look at anti-vaccers’ lists of papers, and see if there are any large, high quality studies.
The largest list (to my knowledge) was compiled by Ginger Taylor and currently contains 157 papers “supporting the vaccine/autism link” (previous versions of the list have contained 91, 124, and 130 papers). There’s also, “30 solid scientific studies that prove vaccines cause autism” and “22 medical studies that show vaccines can cause autism.” All three of these lists have been widely shared so you may find them in different places with different names (as well as older versions with fewer studies), but in my searches, these were the three that I found over and over again. For the most part, they are redundant with each other, but I still painstaking went through them one paper at a time to make sure that I hadn’t missed anything. This produced a total of 160 papers.
To get that number down to something manageable, I did a series of filtering steps to get rid of the papers that weren’t worth talking about (you can download an Excel file showing how I categorized them here). Now, before you accuse me of cherry-picking, please remember that I did the same thing for the pro-vaccine lists. I took lists of over 100 papers, and I wilted them down to just the ones that were worth talking about. Further, as you’ll see in a minute, I was far more generous to the anti-vaccine lists than I was to the pro-vaccine lists. For the pro-vaccine list, I filtered by content, study design, sample size, and study quality. In contrast, for the anti-vaccine lists, I only filtered by content and study design, because if I had filtered by the same sample size and quality standards that I applied to the pro-vaccine lists, I would have had exactly 0 studies left to talk about. In other words, none of the studies on those lists are large, well-conducted studies that used a powerful design and provide good evidence that the current vaccine schedule causes autism.
Note: some of the papers that I am not going to talk about were perfectly fine studies, they just have no relevance to the topic at hand. Many of them were, however, seriously flawed. You can find more details about these studies at I Speak of Dreams. and Stories from the trauma bay.
Note: many papers fit into multiple categories, so if you simply try to add up the numbers from each of the following categories, it is going to look like I suck at math.
Jump back to the top
Studies that weren’t about vaccines or weren’t about autism
It may or may not surprise you to learn that an enormous portion of the papers in these lists had absolutely nothing to do with vaccines and autism. Of the 160 papers in the lists, there were 33 that were not about autism and 82 that were not about vaccines! I’m really curious about how a study that never even uses the words “autism” or “vaccine” can prove that vaccines cause autism. To be clear, I was generous in assigning papers to those categories. I did not score animal studies in that category (even though demonstrating autism in animals is essentially impossible) and I didn’t include papers on thimerosal (even though thimerosal is no longer in childhood vaccines). So right off the bat, we have a really good reason to be skeptical of these lists. They were clearly made by people who are either ignorant or deceptive (or both), because they are full of irrelevant papers.
Just to be clear here, when I say that these papers are irrelevant, for the most part, I mean really well and truly, 100% irrelevant. Some of these papers were so off topic that I have absolutely no clue why they were included. For example, Guy et al. (2015) was on the relationship between pre-term birth and autism, and presented evidence that infants who are born prematurely have a higher risk of developing autism. I have absolutely no clue why Ginger thought that paper was evidence that vaccines cause autism (since it’s not about vaccines), and there were lots of papers like that in the lists. For example, Carvalho et al. 2011 was on methods of treating mercury poisoning. How on earth does a paper on methods for treating mercury poisoning show that vaccines cause autism?
Perhaps most amusingly of all, Ginger’s list includes a few gems like Khaled et al. (2016). This was not about vaccines and never mentioned them. Rather, it looked for biomarkers of autism that were present at birth, and it found them! This study clearly doesn’t suggest that vaccines cause atuism and, in fact, it suggests the opposite. If biomarkers can be used to detect autism at birth (i.e., before vaccines) then clearly vaccines aren’t the problem! I think it is pretty clear that Ginger doesn’t understand the scientific literature.
Other papers were on extremely tangentially related issues. For example, there were several studies on methyl-mercury (e.g., Rice. 1989; Charleston et al. 1994), but methyl-mercury has never been in vaccines. The mercury that used to be in vaccines was ethyl-mercury, which is a very different chemical with different properties. You can’t say, “methyl-mercury does X, therefore ethyl-mercury also does X.” That’s not how chemistry works (also most of those mercury studies weren’t about autism either). Similarly, there were a few papers showing that some component of vaccines were toxic in very high doses, but the dose makes the poison. The fact that chemical Y is dangerous at a very high level is irrelevant to whether or not it is dangerous at the low levels present in vaccines.
Others were about general neurotoxic effects or effects other than autism. Many of these had specific problems that I won’t go into here, but the point that I want to make is that you can’t jump from, “vaccines cause X” to “vaccines cause autism.” Even if these studies had successfully demonstrated that vaccines cause neurological problems other than autism, that wouldn’t indicate or even suggest that vaccines actually cause autism. Each disorder is different with its own set of causes and triggers, and you can’t just assume that the same causal relationships exist for all of them.
The remainder of the studies were, I think, intended to demonstrate various components of hypothetical pathways that supposedly lead from vaccines to autism. For example, there were numerous papers showing associations between oxidative stress and autism, and the argument (I assume) is that vaccines cause oxidative stress, and therefore vaccines can cause autism. There are several problems with that approach, however.
First, the papers on associations between autism and factors other than vaccines were all over the map. They didn’t paint a consistent picture that points towards vaccines. There were studies on associations with the microbiome, associations with oxidative stress, associations with automimue disorders, associations with febrile seizures, associations with mitochondrial disorders, etc. Indeed, Ginger seems to have deluded herself into thinking that any paper on any association with autism is somehow evidence that vaccines cause autism. The list seriously looks like she googled, “causes of autism” then included any studies she found regardless of what it showed.
Second, correlation isn’t causation, and none of those papers established causation, so it could, for example, be the case that some aspect of autism causes oxidative stress rather than the other way around (further, the evidence for vaccines causing oxidative stress is extremely weak).
To put this another way, what the anti-vaccers are doing is laying out a hypothetical pathway in which, for example, they argue that vaccines cause oxidative stress which in turn causes autism, but we don’t know if either of those steps are actually true. Further, even if each step was true independently, you couldn’t actually assume that one will lead to the other in actual patients. The human body is remarkably complex, and biochemical pathways and interactions are complicated and difficult to predict. So it’s often the case that under the right circumstances, A causes B, and under the right circumstances B causes C, but that doesn’t necessarily mean that A will go all the way to C in an actual person.
Finally, and most importantly, in science, you use hypothetical pathways to design experiments, but the pathway itself is not evidence. In other words, you do large studies to see whether or not the pathway is true, and, in the case of vaccines, if this hypothetical pathway actually worked, then the large case-controlled and cohort studies should have found a significant difference between vaccinated and unvaccianted children, but they didn’t. You absolutely cannot present a hypothesis as evidence for your position, but that is exactly what is happening here. These hypotheses have been thoroughly refuted by the large studies that I discussed earlier, and, therefore, they must be rejected.
Jump back to the top
In vitro trials and animal studies
The anti-vaccine lists contained 24 animal studies and 17 in vitro studies (in vitro studies are done on cells and tissues in a petri dish; one study used both methods). There are two important reasons why I am filtering these out (remember that I also eliminated animal trials and in vitro trials from the pro-vaccine lists).
First, and most importantly, these types of studies are always at the bottom of the evidence pyramid. The human body is obviously vastly more complicated than a dish of cells, and in the human body, there are far more chemicals for a drug to interact with, not to mention the fact that you have the kidneys and liver which are actively filtering harmful compounds from your body. As a result, it is very often the case that a chemical will behave one way when directly exposed to a plate of cells (such as nerve cells), but behave very differently in the body where it must travel to the cells without being filtered out or becoming overly diluted, avoid interacting with other chemicals, etc. Similarly, humans, mice, monkeys, etc. are all biochemically different, and chemicals don’t always behave the same way in each species.
Because of all of these factors, in vitro studies and animal trials are preliminary studies that are used as a first pass filtering mechanism. In other words, they are used to decide which topics merit further research, and you absolutely cannot use them as evidence against large epidemiological trials. When an animal trial says X and a cohort study says Y, you go with the cohort study (unless, of course, you can actually find real problems with the cohort study).
The second reason that I am filtering out these trials is that they have very limited applicability to the topic of autism. You cannot diagnose a petri dish as having autism. The best you could do is say, “after being exposed to chemical X, the cells had characteristics that were similar to those of an autistic patient,” but again, association is not causation. So unless you know that those cellular characteristics cause autism, you can’t really say much. Further, showing that a chemical damages a nerve cell does not mean that it will specifically cause autism. Similarly, how would you diagnose autism in a rat? You can say, “the rat is behaving differently,” but again that doesn’t necessarily mean that it specifically has autism.
Finally, I do want to make a few brief comments about a particular set of monkey trials. Anti-vaccers are very fond of citing Hewitson et al. (2008) and Hewitson et al. (2010), which claimed to find evidence of vaccines causing neurological damage in rhesus macaques (anti-vaccers also sometimes cite Hewitson et al. 2009, but that study was withdrawn). All of these were preliminary studies based on ongoing research. Hewitson et al. 2010 literally has the words “pilot study” in the title, and Hewitson et al. 2008 was a conference abstract, not a peer-reviewed paper. Further, the sample sizes were laughably small.
The full study with a more proper sample size has finally come out, and, as often happens in science, the preliminary data were wrong. In the full study, there was no evidence of vaccines causing neurological problems (Gadad et al. 2015). Also, it is worth mentioning that Hewitson is an author on the Gadad paper, and, amusingly, the study was actually funded by an anti-vaccine group!
Jump back to the top
Mercury and thimerosal studies
Mercury is by far the most common vaccine component to be accused of causing autism. Therefore, it should not be surprising that 60 of the papers were specifically about it. However, I’m am not going to talk much about those papers for several reasons.
First, many of these papers were on elemental mercury (Hg) or methyl-mercury, but the preservative used in some vaccines (thimerosal) is actually ethyl-mercury. The mercury in thimerosal does not behave like other types of mercury because it is bound to a ethyl group (just like the chlorine in table salt does not behave like chlorine because it is bound to sodium; details here).
Second, even for the studies on thimerosal, none of them were large human trials that were capable of establishing causation. There were lots of small trials, animal trials, in vitro trials, association studies, etc., but large cohort studies were completely lacking. In contrast, remember that several of the papers in the pro-vaccine list specifically looked at thimerosal (as well as the whole vaccine) and failed to find any relationship. These pro-vaccine studies included a meta-analysis with 1.2 million children (Taylor et al. 2014), a cohort study with 446,695 children (Hviid et al. 2003), another cohort study with 124,170 children (Verstraeten et al. 2003), and a case-controlled trial with over 1,000 children (Price et al. 2010; several of the other studies also used vaccines that contained thimerosal, but they did not explicitly test that component). These massive, high quality studies completely obliterate the small low quality studies presented by the anti-vaccers. That is how the hierarchy of evidence works.
Finally, and perhaps most importantly, most industrialized countries do not currently have thimerosal in their childhood vaccines, and thimerosal has been absent for nearly 20 years (depending on the country)! In the USA, Canada, and countries in the EU, for example, currently only certain strains of the flu vaccine contain thimerosal. Similarly, in Australia it is absent from all childhood vaccines except for certain Hep B vaccines.
This removal of thimerosal is important for two important reasons. First, if you live in a developed country (which is where most of my readers are) then thimerosal in childhood vaccines is a non-issue for you. Even if early exposure to thimerosal did cause autism (which it doesn’t), thimerosal isn’t in childhood vaccines, so you have nothing to worry about.
Second, the nearly world-wide removal of thimerosal from vaccines provides an excellent test of the hypothesis. If thimerosal in vaccines was actually causing autism, then there should have been an obvious drop in autism rates following its removal, but there wasn’t (Madsen et al. 2003; Schechter and Grether 2008). Look at the autism rates over time for any of these countries, and you will not find a noticeable difference following the removal of thimerosal. That is extremely clear evidence that thimerosal does not cause autism.
Now, you may protest and say, “but aren’t trace amounts of it still present in some vaccines?” Yes, trace amounts are present in some vaccines, but think about what you just said, “trace amounts are present.” We are talking about less than 1 microgram of thimerosal per dose. Let me put that in perspective, a small paper clip weighs about 1,000,000 micrograms! We are talking about a dose that is much smaller than any study has ever found to be harmful, and, of course, the dose makes the poison. Finally, if thimerosal caused autism, then the shift to only trace amounts in a few vaccines should still have resulted in lower autism rates.
To quote Orac/Monty Python,
“The hypothesis that mercury in vaccines causes autism is about as dead a hypothesis as there can be. It’s passed on. The hypothesis is no more. It has ceased to be! It’s expired and gone to meet its maker. It’s a stiff. Bereft of life, it rests in peace. It’s shuffled off this mortal coil, run down the curtain and joined the bleedin’ choir invisible! This is an ex-hypothesis!”
Jump back to the top
Conference abstracts, case series opinions, other non-research
The lists contained several conference abstracts (which should always be considered preliminary and should not be used as evidence), case reports/series (which are glorified collections of anecdotes, and anecdotes aren’t evidence of causation), opinion papers, and other non-research papers (such as a bizarre, non-peer-reviewed student paper on court cases [Holland et al. 2011]).
I do, however, want to briefly talk about one of the case reports, because it is very famous in anti-vaccine circles. I am, of course, referring to Poling (2006). The paper documents the story of a girl who developed normally until she received a vaccine, then she regressed into autism. So it is every anti-vaccer’s story, just published in a scientific paper. However, the fact that it was published does not make a causal conclusion any more legitimate than if someone had said it on the internet. Saying, “X happened before Y, therefore X caused Y” is a logical fallacy known as post hoc ergo propter hoc. It does not prove or even suggest that X caused Y. There are also some other really disturbing aspects of this paper. For example, the subject of this study was Hannah Poling. That’s right, she is the author’s daughter (conflict of interest anyone?). In my opinion, parents publishing about their children’s health is probably not a great idea, especially when that parent proceeds to seek a financial settlement for their child’s health (as happened in this case).
Jump back to the top
Actual human studies on current vaccines and autism
After all of that filtering, we are down to just 14 studies and 8 non-systematic reviews that are actually on humans and are relevant to both autism and the current vaccine schedule. So let’s look at them. Some of these are grouped together, and I have preceded each cluster with the title(s) of the paper(s) contained therein (titles are underlined and in quotes).
“A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population”
“Empirical data confirm autism symptoms related to aluminum and acetaminophen exposure”
“Impact of environmental factors on the prevalence of autistic disorder after 1979”
“A comparison of temporal trends in United States autism prevalence to trends in suspected environmental factors”

Correlation does not equal causation. Organic food sales and autism rates are tightly correlated, but that does not mean that organic food causes autism. Image via the Genetic Literacy Project
First, I want to talk about DeLong (2011), Seneff et al. (2012), Deisher et al. (2014), and Nevison (2014). These four were association studies that looked for correlations between autism rates and vaccinations rates. That’s automatically a problem, because association does not mean causation, so even if these studies were good, they would not present evidence that vaccines cause autism. Also, there are additional problems. For example, the DeLong study used very crude state-wide data, failed to account for all possible confounders, and lumped speech disabilities in with autism for the analysis (more details on the problems with this paper here).
Similarly, Seneff et al. (2012) didn’t actual measure autism rates, but instead looked for mentions of it in the self-reported VAERS database (which went up over time), then tried to match that to the amount of aluminum in vaccines. Because it is self-reported, VAERS is notoriously unreliable for things like this, especially in this case because there is so much evidence that autism rates aren’t actually increasing (Rutter 2005; Taylor 2006; Bishop et al. 2008; Baxter et al. 2015; Hansen et al. 2015). Think about it, autism has become an increasingly hot topic over time, so you would naturally expect it to show up more often in VAERS over time, thus completely negating the study (other problems are described here).
Next, we have Deisher et al. (2014). This study attempted to look for correlations between the release of certain vaccines and increases in autism rates, and it is honestly a very hard paper to read because it is so horrible. The writing is nearly impossible to follow, the methods are nonsense, the statistics are total crap, the conclusions aren’t merited by those statistics, and the fundamental premises of the paper are refuted by numerous other studies (i.e., it assumes that autism rates are actually going up, which, once again, they likely aren’t). In short, what they did was take a data set that would normally be analyzed by linear regression, then chop it up based on cherry-picked data points. Other authors have explained the problems in detail, so I’ll defer to them (here and here).
Finally, we have Nevison (2014). In short, this study claimed to find an increase in autism rates over time (which is debatable), and it found that the increase correlates with glyphosate use and aluminum in vaccines. As illustrated earlier, however, you can also make a nice graph that shows a correlation between autism and organic food sales. Just because two things increase together does not mean that one causes the other. I think that you probably get the picture by now, so I won’t waste any more time on this paper.
“Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? “
Now we arrive at the infamous Tomljenovic and Shaw (2011) study. It’s a paper that is so fundamentally flawed that I don’t even know where to begin, and it would take me an entire (and lengthy) post to go over all of the problems with it. Fortunately, others have done that for me, so I will defer you to them and just hit the highlights.
First, this study looked at two regressions: autism and aluminum in the US, and autism and aluminum across countries. We have lots of problems here. First, as Orac explains in more detail, you have a problem known as an ecological fallacy where you lump a very large data set (i.e., a country) into a single data point. In other words, they aren’t showing that individuals who receive vaccines have higher autism rates. Rather, they are showing that countries with lots of vaccines have higher autism rates. That is a huge problem because there are obviously tons of factors other than just vaccination rates that differ among countries (which means that we can’t be sure that vaccines are the thing that is causing the difference in autism rates). Additionally, as explained here, the sources of the data for different countries varied widely and involved different cohorts, and it appears that the authors cherry-picked their sources.
Even if we zoom in on the correlation in the US, we have serious problems. To assess autism rates, they looked at the number of autistic children who were reported via the Individuals with Disabilities Education Act (IDEA) database, which is an extremely problematic and inappropriate way to measure autism levels because it is affected by diagnostic changes, and, once again, the increase in autism seems to be largely due to diagnostic changes rather than actual changes (Rutter 2005; Taylor 2006; Bishop et al. 2008; Baxter et al. 2015; Hansen et al. 2015).
Finally, this is yet another association study. It cannot demonstrate causation, but that doesn’t stop the authors from trying. They misappropriate Hill’s criteria, which is a series of nine diagnostic criteria used to assess whether or not causation is likely. I will outline and discuss them below.
- Strength (robustness): Although they did get low P values, their methods have multiple problems and confounding factors that they did not account for. So this study fails the strength test.
- Consistency (consistent with other results): This study is extremely inconsistent with all of the large studies discussed early.
- Specificity (if you are dealing with a very specific, isolated event, causation is more likely): This was done at the country level. It is as far from specific as you can get.
- Temporality (cause happens before affect): This could not be assessed by this study.
- Biological gradient (i.e., higher dose = stronger effect): This was not evaluated by this study, but I cited several studies earlier that failed to find a relationship between the number of vaccine doses and autism.
- Plausibility: Once upon a time, the vaccine/autism hypothesis was plausible, but now that it has been so thoroughly tested, it is no longer plausible.
- Coherence (agreement of laboratory and epidemiological findings): There are lots of in vitro and animal trials that have found vaccines to be safe.
- Experiment: not relevant for this particular topic
- Analogy: not relevant for this particular topic
It’s pretty obvious that this paper epically fails Hill’s criteria. So, in short, this paper showed some shoddy correlations that were based on crude, inappropriate, and cherry-picked data sources. It absolutely is not evidence that vaccines cause autism.
“Hepatitis B triple series vaccine and developmental disability in US children aged 1-9 years”
“Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997–2002.”
Next, I want to look at two studies by Gallagher and Goodman. Gallagher and Goodman (2008) is another study that used general developmental disorders, rather than autism specifically (which automatically makes it problematic and means that we can’t reach any conclusions specifically about autism). Further, it was yet another association study, and it relied on parental surveys (which are often prone to biases). Additionally, it had fairly small sample sizes (228 unvaccinated boys, 678 vaccinated boys, 217 unvaccinated girls, and 571 vaccinated girls). Most importantly though, its results are entertainingly problematic. It found higher levels of EIS (special education services) in vaccinated boys than unvaccinated boys (7% vs 3%), but it also found significantly lower levels of EIS in vaccinated girls than in unvaccinated girls (2% vs 6%). That is extremely clear evidence that the results of this study are simply statistical noise produced by a weak study design and small sample sizes. To put this another way, if you want to use this study as evidence that vaccines cause autism in boys, you must simultaneously use it as evidence that they prevent autism in girls.
Now, let’s look at Gallagher and Goodman 2010. This was a cross-sectional study, which is a study design that looks at the rate of something in a population, then looks for possible causes of that thing. This is a very weak type of association study which cannot establish causal relationships and is easily biased by numerous factors. Additionally, this study also had a very small sample size of only 31 boys with autism (which is what they used for the stats). The sample for non-autistic children was much higher, but the study is limited by the smallest sample size, and when you couple a weak experimental design with a tiny sample size, you get unreliable results, which is the best word to describe both Gallagher and Goodman studies: “unreliable.”
“Serological association of measles virus and human herpesvirus-6 with brain autoantibodies in Autism”
“Abnormal measles-mumps rubella antibodies and CNS autoimmunity in children with autism”
Next, let’s talk about two papers for which Vijendra Singh was the primary author. First, we have Singh et al. 1998, which is another really sorry excuse for a paper. It is yet another association study, and it also had tiny sample sizes (48 with autism and 43 controls; you should be detecting a theme by now). Most importantly, their numbers are so far off that I am willing to label it “fraudulent.” The authors looked at serum levels of HHV-6-IgG, measles-IgG, anti-MBP, and anti-NAFP, and found that 70% of the autistic children were positive for anti-MBP. Simple math tells us that 70% of 48 is 34 (after rounding). So 34 of their autistic children had anti-MBP; however, in table 1, where they are presenting the “associations” on which their entire paper is based, they reported that 37 autistic children had both measles IgG antibodies and anti-MBP. That is not possible if only 34 autistic children had anti-MBP. Similarly, they said that 57% of autistic children were positive for anti-NAFP. So 57% of 48 is 27 autistic children with anti-NAFP. Yet they claim that 30 autistic children had both measles IgG and anti-NAFP. Whenever you find inconsistencies of this magnitude in the core results of a paper, you should toss out the whole paper, because at that point, you don’t have any reason to trust anything in it. There are also lots of other problems with this study, such as the fact that there was no significant difference in viral levels in the autistic and non-autistic group (which is the opposite of what you would expect if exposure to the virus caused autism), but the numerical inconsistencies are so great that I don’t feel the need to go any further.
The next study from this group, (Singh et al. 2002) also looked at serum levels. Specifically, it was looking for antibodies produced by the MMR vaccine as well as anti-MBP. Once again, it is a small association study (125 autistic children, 92 controls), and the results are, unsurprisingly, a bit suspicious. They used two different techniques for detecting the antibodies, and the main one (which was used for the primary comparisons) found MMR antibodies in 60% of autistic children, or at least that’s what the text says. According to to figure 5, it was only about 55%. Again, inconsistencies like that in the main results are enormous red flags. At best, they mean that the authors were really sloppy (which should make you question every part of the study and analysis), and at worst, they are dishonest and fudged the results. Additionally, this technique did not detect MMR antibodies in any of the control children. This is extremely surprising, because all of the control children were vaccinated, which means that most of them should have had those antibodies. Further, their other technique (which was used on a subset of samples) did detect MMR antibodies in some of the controls, which means that either their primary method was not sensitive enough to be useful, or they lied. Either way, this paper is busted.
“Possible immunological disorders in autism: concomitant autoimmunity and immune tolerance”
Next, I want to talk about Kawashti. (2006). The inclusion of this paper in the anti-vaccers’ list amuses me to no end, because it is designed very similarly to the Singh et al. papers (i.e., it looked for antibodies from the MMR vaccine in children with and without autism), but it found the exact opposite! It found the antigens for measles, mumps, and rubella were present in 100% of non-autistic children, but only 50%, 73.3%, and 53.3% of autistic children. Further, it concluded “At this stage, we can conclude that M.M.R. vaccine may not be a cause of autism.” That’s right, this is not actually an anti-vaccine paper. This, once again, shows just how little quality control went into constructing the anti-vaccine lists. This paper directly contradicts other papers in the list, yet it was still included (note: this is another small association study, so I’m not touting it as evidence that vaccines don’t cause autism; rather, the point is simply that the anti-vaccers screwed up and put a pro-vaccine paper in their list).
“Preterm birth, vaccination and neurodevelopmental disorders: a cross-sectional study of 6- to 12-year-old vaccinated and unvaccinated children”
“Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12- year old U.S. children”
Next, let’s talk about a particularly awful pair of studies: Mawson et al. (2017a, b). These papers aren’t actually published in real, respected journals. Rather, they both appear in the predatory journal, “Journal of Translational Science.” Further, one of them (Mawson et al. 2017a) only appeared there after being retracted from a different journal. Retraction Watch reported that Translational Science was going to retract it as well, but it is currently still available on their site.
Both “studies” are based on an online survey that used a method known as “convenience sampling.” They simply sent the survey to homeschool groups (which tend to be dominated by anti-vaccers), and they did not use any of the controls or randomizations that are neccissary for a proper survey. In statistics courses, literally the first thing that you learn about surveys is that you shouldn’t use convience sampling.
Essentially, what these studies did was poll anti-vaccers about their children’s medical history. Unsurprisingly, when you poll people who are convinced that vaccines cause autsim, you get the result that vaccines cause autism. These papers are complete nonsense (which is why they are in a predatory journal instead of real journals). You can read more about these studies at Science-Based Medicne, Vaccines Work, and Respectful Insolance.
“Can awareness of medical pathophysiology in autism lead to primary care autism prevention strategies?”
Now, I want to shift gears a bit and talk about Mumper (2013). This is a truly bizarre “study.” It was published in the North American Journal of Medicine and Science, which is a journal that is so minor that I couldn’t even find an impact factor (in laymen’s terms, that means that no one cites this journal or takes it seriously). Further, the paper itself doesn’t follow any of the standard conventions for a scientific paper (it includes bizarre sections like anecdotes of the author’s travels to other countries). It looks more like an undergraduate report than a scientific paper.
It may seem like I am being nitpicky, but all of those things are actually clues that this is a subpar paper that did not go through a proper review process. You should learn to watch out for flags like that as you read scientific papers. Then, of course, we have the actual experimental design (and I’m using that term very loosely). The author works at a private pediatric clinic that stresses a lot of different things like breastfeeding, probiotics, nutritional counseling, flexible vaccine schedules, etc. Some of those are good, some are bad, but what she did, was go back through her records since 2005 to see if any of their infants had been diagnosed with autism while under their care. She found that out of 294 infants, none had been diagnosed with autism. This is lower than the national background rate of 1 in 59, so she made an astronomical jump to the conclusion that her clinic’s practices prevent autism (or at least avoid the causes of autism). That’s clearly an absurd conclusion. What she did is not even close to a proper study. Nevertheless, let’s assume for a second that it was. Let’s assume that there is actually something happening at that clinic that prevents autism. You still can’t jump to the conclusion that it was vaccines because there are so many factors. Maybe it was breastfeeding. Maybe it was probiotics, etc. This is not a real study. It is an anecdote that has been dressed up as a study.
“Detection and sequencing of measles virus from peripheral mononuclear cells from patients with inflammatory bowel disease and autism.”
Kawashima et al. (2000) simply found DNA from the measles vaccine in the colons of nine autistic patients, which of course doesn’t mean anything other than that DNA from the measles vaccine was in their colons. That result is not even remotely evidence that the vaccine does anything harmful.
“Epidemiologic and molecular relationship between vaccine manufacture and autism spectrum disorder prevalence.”
This paper (Deisher et al. 2015) was thoroughly debunked on Science-Based Medicine, so I will defer to that post, but in short, it is on an implausible hypothesis, the data were collected in a very questionable way, and the data were presented deceptively to show trends that aren’t really there. Additionally, this paper was on the MMR vaccine, which is also the vaccine that was specifically examined by most of the large cohort studies, the massive meta-analysis, etc. All of those studies were far more powerful than this study, so you really can’t use this paper as evidence that those papers are wrong. Finally, this paper was published in an extremely minor journal (the impact factor is roughly 0), which is a huge red flag that it is junk science.
Note: This paper was not in any of the anti-vaccine lists so it is not included in the paper count, but I have seen anti-vaccers citing it elsewhere, so I have included it here
Jump back to the top
Reviews
At this point, I have gone through the relevant anti-vaccine literature and showed that all of the studies are small and incapable of demonstrating causation, and I have showed that many of them are riddled with problems. So you may be wondering, “what could the reviews possibly be on?” Well this is where we come back to the importance of systematic reviews. If you recall in the pro-vaccine section, all of the reviews that I cited were systematic, meaning that they used pre-defined search terms and criteria. The anti-vaccine reviews, however, are not systematic. Thus, they completely ignored all of the large studies that have discredited the vaccine/autism hypothesis, they ignored all of the problems with the anti-vaccine studies, and they used all of those tiny, problematic studies to spin a fanciful tale in which, through a complex, unlikely, and thoroughly discredited series of events, vaccines cause autism. In other words, all that these “reviews” do is set forth a hypothesis. Doing that would be fine if it wasn’t for the fact that the hypothesis has been discredited by numerous massive studies. Again, you always reject a hypothesis based on the evidence. You never reject the evidence based on a hypothesis, but that is exactly what these papers are doing. They are deceptively only showing the papers that support their position while ignoring all of the papers that refute it.
Here is the list of reviews: Rimland and McGinnis. 2002, Singh. 2009, Ratajczak 2011 (details of problems here and here), Sienkiewicx et al. 2012 (details of problems here) Shaw and Tomljenovic. 2013b, Shaw et al. 2014a, Morris et al. 2017a and Lyons-Weiler 2018 (details of problems here). Most of these contain numerous blatantly false (or at least highly misleading) statements, but the main point that I want to drive home is simply that they are stating hypotheses rather than presenting evidence of causation, and they are ignoring the fact that those hypotheses have already been tested and refuted.
Note: to be fair, Rimland and McGinnis (2002) was written before the large studies were available, so they were stating a hypothesis that had yet to be thoroughly tested, which is fine, but most of these reviews were written after the hypothesis had been thoroughly refuted.
Note: There were actually 37 reviews in all, but most of them were not about vaccines, were about thimerosal, etc. So only the eight listed here were actually relevant for the current vaccine schedule.
Jump back to the top
Conflicts of interest
Anti-vaccers are very quick to point out conflicts of interest in pro-vaccine papers (or, more often, assume that they exist before they even check for them), but they are very slow to acknowledge them in their own papers. So I want to briefly provide a few examples to show that they do in fact exist (I did not check for conflicts in all of the anti-vaccine papers).
First, it is worth mentioning that this whole vaccine/autism mess got started when Andrew Wakefield falsified evidence against the MMR vaccine and conspired with lawyers to sue pharmaceutical companies, all while covertly working on a patent for his own vaccine which he planned to replace the MMR vaccine with (details here and here). Similarly, Geier, who is the author of a case series that anti-vaccers love to cite (Geier and Geier 2007) as well as several other anti-vaccine studies, has had his medical license suspended for unethical behavior and, “incompetence or multiple instances of negligence.” The heroes of the anti-vaccine movement leave much to be desired. Further, those two are far from alone. As I mentioned earlier, Dr. Poling published his infamous case report while in the process of seeking a financial settlement for his daughter’s “vaccine injury.”
Dr. Shaw and Dr. Tomljenovic are also two fantastic examples of conflicts of interest. These are two of the most prominent anti-vaccine scientists, and eight of the papers in the anti-vaccers’ lists were authored by at least one of them. However, both of them have served as consultants or expert witnesses in vaccine lawsuits, Shaw is the chair of the Scientific Advisory Board for an anti-vaccine group, and at least one of their studies was funded by members of the governing board of that group (more info here). Funding from an activist group that describes vaccines as, “a holocaust of poison on our children’s brains and immune systems” is just as big of a conflict of interest as funding from a pharmaceutical company. So, according to standard anti-vax reasoning, this should cast doubt on all of the authors’ work.
Similarly, Dr. Singh (who you may remember authored two of the papers and one of the reviews that I talked about) was funded by the Autism Research Institute, which, at the time that he received funding, ran a program called “Defeat Autism Now!,” which actively promoted the idea that vaccines cause autism. Further, remember that horrible DeLong (2011) paper that I talked about earlier? Well DeLong is a board member of the prominent anti-vaccine group “SafeMinds,” and, like Poling, is the parent of an autistic child. Similarly, those Mawson surveys I talked about were funded by Generation Rescue, yet another anti-vaccine organization.
I could keep going, but I think that I have made my point clear. Anti-vaccers like to pretend that all of their studies are conflict free and represent true, unbiased research. In reality, there are plenty of anti-vaccine organizations that are happy to fund anti-vaccine studies, and many of the authors are deeply involved in the anti-vaccine movement. To be clear, I’m not suggesting that we should automatically reject these papers because of those conflicts (we should reject them because they are junk science), but I wanted to point out that, despite what anti-vaccers like to think, they are not free from conflicts of interest.
Note: please see these two posts for more info on when and how it is OK to attack a source.
Studies that I did not include
You may have noticed that I did not talk about either the original Wakefield study or Hooker (2014). That is because both of these studies were so flawed that they were retracted (I talked more about Hooker’s study here).
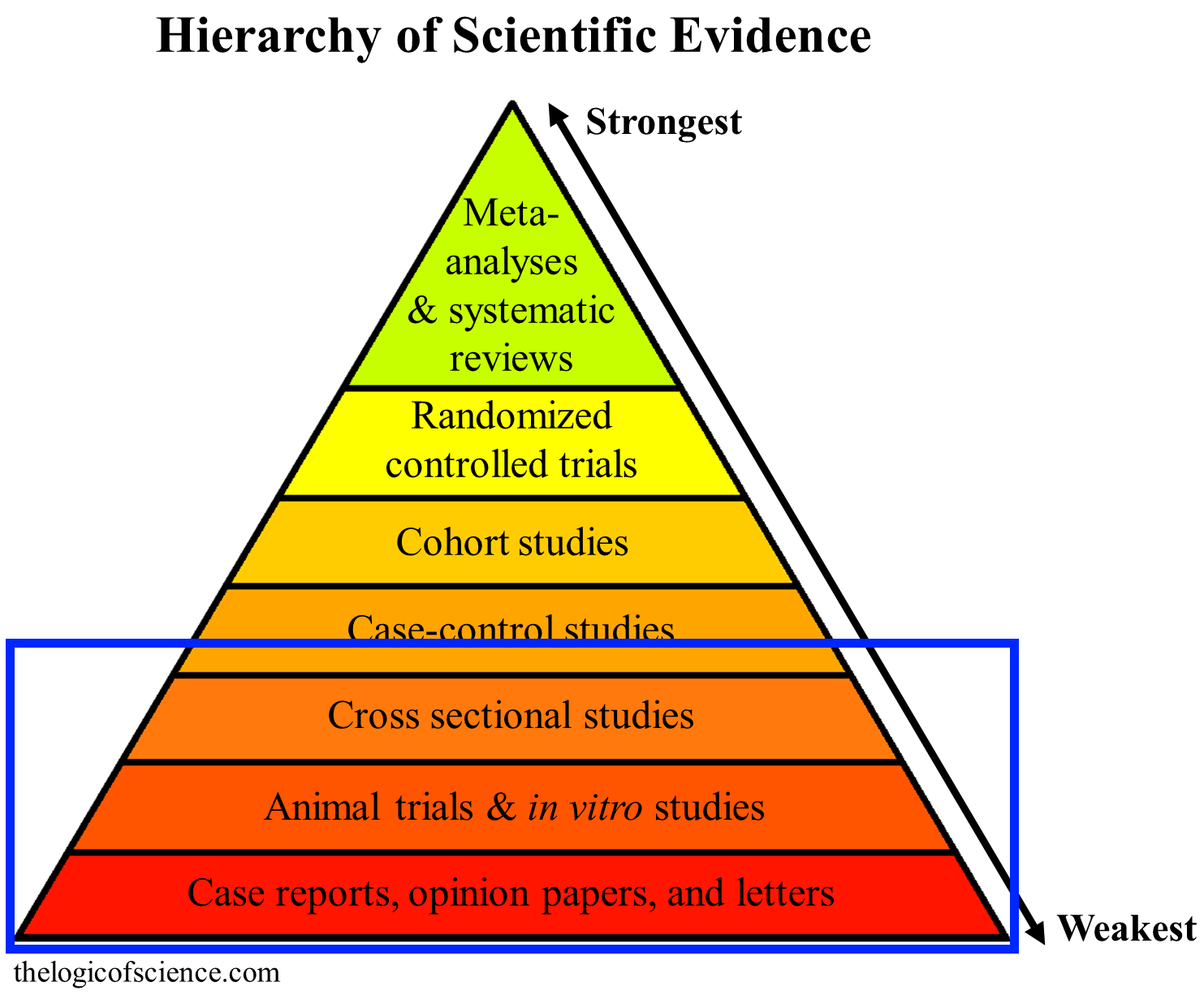
All of the anti-vaccine papers fell into the lowest categories of evidence, and none of them were capable of showing causal relationships (details here).
Overview of anti-vaccine papers
In short, the vast majority of papers cited by anti-vaccers aren’t even about vaccines and autism. Of the ones that are, many of them are animal trials and in vitro trials, or they are about thimerosal, which is no longer in vaccines and has been documented to be safe via several very large epidemiological studies. Indeed, there were only 14 studies on humans that were about both vaccines and autism and were relevant to the current vaccine schedule, but none of them were case-controlled or cohort studies, and there were no meta-analyses or systematic reviews. The studies used small sample sizes and shoddy statistics to show crude correlations, and none of them had the ability to assign causation. Further, most of them were filled with problems, and one of them was actually a pro-vaccine paper. There were also eight non-systematic reviews, but these were essentially glorified opinion papers that ignored all of the literature against a link between autism and vaccines. They simply presented hypotheses rather than evidence, and those hypotheses have been thoroughly discredited by large studies.
Jump back to the top
Anecdotes, Court Cases, VAERS, etc.
At this point, it should be exceptionally clear that there is no good scientific evidence to suggest that vaccines cause autism, which means that this is usually the point at which people start trying to use non-scientific evidence. Therefore, I want to very briefly explain the problems with some common non-scientific arguments.
The most common response to the statement, “vaccines don’t cause autism” is probably the appeal to anecdotes. The internet is full of stories of people who vaccinated their child, then watched as the child regressed. The problem is, of course, that anecdotes aren’t evidence. The fact that X happened before Y does not mean that X caused Y. In fact, arguing that X caused Y is a logical fallacy known as post hoc ergo propter hoc. This is especially true for something like autism because the first signs of autism usually appear around the same age as many vaccinations. Therefore, given the large number of people who develop autism, and the large number of people who are vaccinated, you expect there to be many cases where vaccination and the onset of autism occur together just by chance. Really think about that for a minute. If 1 in 59 children will have autism, usually with the first obvious symptoms occurring around 2-3 years of age, and over 90% of children receive vaccines around 2-3 years of age, then there should be lots of cases where parents notice the signs of autism shortly after vaccinating, even if vaccines aren’t the cause (I actually ran the numbers on this here).
I fully understand why parents would blame vaccines. I understand why seeing your child develop autism shortly after receiving a vaccine would make you think that the vaccine was responsible, but you need to realize that lots of things happen together just by chance, and, as a result, anecdotes are not valid evidence. If vaccines actually did cause autism at the rates claimed by anti-vaccers, then the large, systematic studies should have found a significant difference between vaccinated and unvaccinated children. In the face of evidence like that, it is not logically or scientifically valid to cling to anecdotes.
An extension of the anecdote argument is to cite reports of vaccines causing autism in the Vaccine Adverse Event Reporting System (VAERS). VAERS is, however, a self reported database. In other words, it is just a collection of anecdotes. The fact that someone reported an anecdote to VAERS doesn’t make the anecdote any more trustworthy than if it was on Facebook. The point of databases like this is to allow doctors and scientists to identify potential issues that need to be studied. It is not meant to be used as evidence of causation (more details about issues with using VAERS as evidence here and here).
A final line of anecdotal reasoning involves appealing to the vaccine package inserts (which is the one and only time that anti-vaccers trust pharmaceutical companies). The problem is, once again, that the lists of adverse reactions do not demonstrate causation. Those lists consist of any symptoms reported during clinical trials, most of which were almost certainly not caused by the vaccine. In fact, the package inserts even state that the list of adverse reactions is not a list of confirmed causal relationships.
Another common strategy is to appeal to court cases. There have been various court cases in various countries where money has been awarded to people who claim that vaccines gave their child autism (there have also been plenty that were thrown out of court or later overturned). To anti-vaccers, these are admissions of guilt by governments and confirm that vaccines are dangerous. In reality, they are nothing of the kind. The fact that a judge concluded that a vaccine caused autism does not mean that the vaccine actually did cause autism. This is a blatant appeal to authority fallacy. Judges aren’t infallible, and they usually aren’t even scientists. A judge can be deceived about the current state of our scientific knowledge just as easily as anyone else. So you absolutely cannot say, “This court gave money for an autism case, therefore all of those massive studies with hundreds of thousands of children must be wrong.” Hopefully you can see why statements like that are absurd (more on why court cases shouldn’t be used as scientific evidence here).
Additionally, there has been a great deal of fuss over the “CDC whistleblower.” I won’t go into the details because it is just too long of a story, but the short version is that there was no cover up and the CDC did not hide evidence or deceive the public. This argument is nothing more than typical conspiracy theorist ramblings. Many others have explained the situation in detail, so if you are prone to using this argument, please see their posts (for example, here, here, and here).
Finally, when faced with the overwhelming evidence that vaccines are safe, many people try to argue that science shouldn’t be trusted because it has been wrong before (debunked here) or by citing the work of Dr. Ioannidis and claiming that most studies are wrong, therefore we can blindly ignore the studies on vaccine safety (debunked here). Both of these arguments are logically and scientifically invalid. The fact that science has been wrong before doesn’t mean that you can dismiss it anytime that you want to. Similarly, what Ioannidis’s work actually shows is exactly what I have argued in this post: on any topic there will be many small, poorly conducted, and unreliable studies, so we have to really on a consensus of large, high-quality studies.
Conclusion
If you made it all the way here, then congratulations on reading the world’s longest blog post (or at least an unusually long post). It should now be clear to you that the evidence really is overwhelmingly supportive of vaccines. Even though anti-vaccers claim to have lengthy lists of papers supporting their position, most of those papers are irrelevant, used weak designs, and had small sample sizes. In contrast, the literature supporting vaccine safety consists of multiple exceptionally large and powerful studies. So there really is no good scientific evidence to suggest that vaccines cause autism.
Jump back to the top
Literature Cited
- Akinrinade et al. 2015. Interplay of glia activation and oxidative stress formation in fluoride and aluminium exposure. Pathophysiology 22:39–48.
- Anders et al. 2004. Thimerosal exposure in infants and developmental disorders: a retrospective cohort study in the United Kingdom does not support a causal association. Pediatrics 114:584–591
- Austin and Shandley. 2008. An investigation of porphyrinuria in Australian children with autism. J Toxicol Environ Health A 71:1349–1351
- Baxter et al. 2015. The epidemiology and global burden of autism spectrum disorders. Psychological Medicine 45:601–613
- Bernard et al. 2001. Autism: a novel form of mercury poisoning. Medical Hypotheses 56:462–471.
- Bishop et al. 2008. Autism and diagnostic substitution: evidence from a study of adults with a history of developmental language disorder. Dev Med Child Neurol 50: 341–345
- Blaurock-Busch et al. 2012. Toxic metals and essential elements in hair and severity of symptoms among children with autism. Maedica 7:38–48
- Blaxill. 2004. What’s going on? The question of time trends in autism. Public Health Rep. 119:536–551
- Blaxill et al. 2003. Commentary on Croen et al. (2002), The Changing Prevalence of Autism in California. J Autism Dev Disord. 223–226
- Blaxill et al. 2004. Thimerosal and autism? A plausible hypothesis that should not be dismissed. Med Hypotheses 62:788–794
- Branch. 2009. Gender-selective toxicity of thimerosal. Exp Toxicol Pathol 61:133–136
- Breecea et al. 2013. Myeloid dendritic cells frequencies are increased in children with autism spectrum disorder and associated with amygdala volume and repetitive behaviors. Brain Behav Immunity 31:69–75
- Brown et al. 2014. Elevated maternal C-reactive protein and autism in a national birth cohort. Mol Psychiatry 19:259–264
- Burbacher. 2005. Comparison of blood and brain mercury levels in infant monkeys exposed to methylmercury or vaccines containing thimerosal. Environ Health Perspect 113:1015–1021
- Carvalho et al. 2008. Inhibition of the human thioredoxin system. A molecular mechanism of mercury toxicity. J Biol Chem 283:11913-11923
- Carvalho et al. 2011. Effects of selenite and chelating agents on mammalian thioredoxin reductase inhibited by mercury: implications for treatment of mercury poisoning. FASEB J 25:370–381
- Charleston et al. 1994. Increases in the number of reactive glia in the visual cortex of Macaca fascicularis following subclinical long-term methyl mercury exposure. Toxicol Appl Pharmacol 129:196–206
- Chauhan and Chauhan. 2006. Oxidative stress in autism. Pathophysiology 13:171–181
- Chen et al. 2004. No evidence for links between autism, MMR and measles virus. Psychol Med 34:543–553
- Chen et al. 2013. Effect of thimerosal on the neurodevelopment of premature rats. World J. Pediatr. 9:356–360.
- Cheuk and Wong. 2006. Attention-deficit hyperactivity disorder and blood mercury level: a case-control study in Chinese children. Neuropediatris 37:234–240
- Christian et al. 2011. Inflammatory responses to trivalent influenza virus vaccine among pregnant women. Vaccine 29:8982–8987
- Dales et al. 2001. Time trends in autism and in MMR immunization coverage in California. JAMA 285:1183–1185
- Deisher et al. 2014. Impact of environmental factors on the prevalence of autistic disorder after 1979. J Public Health Epidemiol 6:271–286
- Deisher et al. 2015. Epidemiologic and molecular relationship between vaccine manufacture and autism spectrum disorder prevalence. Issues in Law and Medicine 30:47-70.
- DeLong. 2011. A positive association found between autism prevalence and childhood vaccination uptake across the U.S. population. J Toxicol Environ Health A 74:903-916
- Demicheli et al. 2012. Vaccines for measles, mumps and rubella in children. Cochrane Database Syst Rev
- DeStefano et al. 2004. Age at first measles-mumps-rubella vaccination in children with autism and school-matched control subjects: a population-based study in metropolitan Atlanta. Pediatrics 113:259–266
- DeStefano et al. 2013. Increasing exposure to antibody-stimulating proteins and polysaccharides in vaccines is not associated with risk of autism. J Ped 163:561–567
- Desoto and Hitlan. 2007. Blood levels of mercury are related to diagnosis of autism: a reanalysis of an important data set. J Child Neurol 22:1308-1311
- Desoto and Hitlan. 2010. Sorting out the spinning of autism: heavy metals and the question of incidence. Acta Neurobiol Exp 70:165–176
- Dickerson et al. 2015. Autism spectrum disorder prevalence and proximity to industrial facilities releasing arsenic, lead or mercury. Sci Total Environ 536:245–251
- Dórea. 2011. Integrating experimental (in vitro and in vivo) neurotoxicity studies of low-dose thimerosal relevant to vaccines. Neurochem Res 36:927–938
- Duszczyk-Budhathoki et al. 2012. Administration of thimerosal to infant rats increases overflow of glutamate and aspartate in the prefrontal cortex: protective role of dehydroepiandrosterone sulfate. Neurochem 37:436–447
- Ekstrand et al. 2010. Mercury toxixokenetics—dependency on strain and gender. Toxicol Appl Pharmacol 15:283–291
- Elsabbagh et al. 2012. Global prevalence of autism and other pervasive developmental disorders. Autism Research 5:160–179
- Ercal et al. 2001. Toxic metals and oxidative stress part 1: mechanisms involved in metal induced oxidative stress. Curr Top Med Chem 1:529–539
- Eshraghi et al. 2018. Early Disruption of the Microbiome Leading to Decreased Antioxidant Capacity and Epigenetic Changes: Implications for the Rise in Autism. Front Cell Neurosci
- Ewing. 2009. What is regressive autism and why does it occur? Is it the consequence of multi-systemic dysfunction affecting the elimination of heavy metals and the ability to regulate neural temperature? N AM J Med Sci 1:28–47
- Feenstra et al. 2014. Common variants associated with general and MMR vaccine-related febrile seizures. Nat. Genet. 46:1274–1282
- Fiorentino et al. 2016. Blood–brain barrier and intestinal epithelial barrier alterations in autism spectrum disorders. Molecular Autism 7:49
- Fombonne et al. 2006. Pervasive Developmental Disorders in Montreal, Quebec, Canada: Prevalence and Links With Immunizations. Pediatrics 118
- Gagag et al. 2015. Administration of thimerosal-containing vaccines to infant rhesus macaques does not result in autism-like behavior or neuropathology. PNAS 112: 12498–12503
- Gallagher and Goodman. 2008. Hepatitis B triple series vaccine and developmental disability in US children aged 1-9 years. Toxicol Environ Chem 90:997–1008
Gallagher and Goodman. 2010. Hepatitis B vaccination of male neonates and autism diagnosis, NHIS 1997–2002. J Toxicol Environ Health A 73:1665–1677 - Gargus and Imtiaz. 2008. Mitochondrial energy-deficient endophenotype in autism. Am J Biochem Biotech 4:198–207
- Gesundheit et al. 2013. Immunological and autoimmune considerations of Autism Spectrum Disorders. J. Autoimmun 44:1–7
- Geier and Geier. 2007. A case series of children with apparent mercury toxic encephalopathies manifesting with clinical symptoms of regressive autistic disorder. J Toxicol Environ Health A 15:837–851
- Ghanizadeh et al. 2012. Glutathione-related factors and oxidative stress in autism, a review. Curr Med Chem 19:4000–4005
- Goin-Kochel et al. 2016. Parental report of vaccine receipt in children with autism spectrum disorder: Do rates differ by pattern of ASD onset? Vaccine 34:1335–1342.
- Gorrindo et al. 2013. Enrichment of elevated plasma F2t-Isoprostane levels in individuals with autism who are stratified by presence of gastrointestinal dysfunction. PLoS ONE 8:e68444
- Goth 2006. Uncoupling of ATP-mediated calcium signalling and dysregulated interleukin-6 secretion in dendritic cells by nanomolar thimerosal. Environ Health Perspect 114:1083–1091
- Griffiths and Levy. 2017. Evidence of Mitochondrial Dysfunction in Autism: Biochemical Links, Genetic-Based Associations, and Non-Energy-Related Mechanisms. Oxid Med Cell Longev 2017:4314025
- Gupta. 2014. Transcriptome analysis reveals dysregulation of innate immune response genes and neuronal activity-dependent genes in autism. Nat Commun 5:5748
- Guy et al. 2015. Infants born late/moderately preterm are at increased risk for a positive autism screen at 2 years of age. J. Pediatr 166:269–275
- Haley 2005. Mercury toxicity: Genetic susceptibility and synergistic effects. Medical Veritas 2:535-542
- Hamza et al. 2012. Hepatitis B vaccine induces apoptotic death in Hepa1-6 cells. Apoptosis 17:516–527
- Hansen et al. 2015. Explaining the increase in the prevalence of autism spectrum disorders: the proportion attributable to changes in reporting practices. JAMA Pediatrics 169:56–62
- Herbert. 2005a. Autism: a brain disorder, or a disorder that affects the brain? Clinical Neurophsychiatry 2:354–379
- Herbert. 2005b. Large brains in autism: the challenge of pervasive abnormality. Neuroscientist. 11:417–40
- Hertz-Picciotto and Delwiche. 2009. The rise in autism and the role of age at diagnosis. Epidemiology 20:84–90
- Herdman et al. 2006. Thimerosal induces apoptosis in a neuroblastoma model via the cJun N-terminal kinase pathway. Toxicol Sci 92:246–253
- Hewitson et al. 2008. Pediatric vaccines influence primate behaviour and amygdala growth and opioid ligand binding. International Meeting for Autism Research
- Hewitson et al. 2010. Influence of pediatric vaccines on amygdala growth and opioid ligand binding in rhesus macaque infants: A pilot study. Acta Neurobiol Exp 70:147–164
- Hviid et al. 2003. Association between thimerosal-containing vaccine and autism. JAMA 290:1763–1766
- Hviid et al. 2019. Measles, mumps, rubella vaccination and autism: A nationwide cohort study. Annals of Internal Medicine.
- Holland et al. 2011. Unanswered questions: A review of compensated cases of vaccine-induced brain injury. Pace Environmental Law Review 28:2
- Holmes. 2003. Reduced levels of mercury in first baby haircuts of autistic children. Int J Toxicol 22:277–285
- Honda et al. 2005. No effect of MMR withdrawal on the incidence of autism: a total population study. J Child Psych and Psychiat 46:572–579
- RETRACTED Hooker. 2014. Measles-mumps-rubella vaccination timing and autism among young African American boys: a reanalysis of CDC data. Translational Neurodegeneration 3:16
- Howsmon et al. 2017. Classification and adaptive behavior prediction of children with autism spectrum disorder based upon multivariate data analysis of markers of oxidative stress and DNA methylation. PLoS Computational Biology
- Howsmon et al. 2018. Multivariate techniques enable a biochemical classification of children with autism spectrum disorder versus typically‐developing peers: A comparison and validation study. Bioengineering and Translational Medicine 3:156–165.
- Humphrey et al. 2005. Mitochondrial mediated thimerosal-induced apoptosis in a human neuroblastoma cell line (SK-N-SH). Neurotoxicology. 26:407–416
- Hurley et al. 2010. Thimerosal-containing vaccines and autism: a review of recent epidemiologic studies. J. Pediatr Pharmacol Ther 15:173–181
- WITHDRAWN Inbar, et al. 2016. Behavioral abnormalities in young female mice following administration of aluminium adjuvants and the human papillomavirus (HPV) vaccine Gardasil. Vaccine
- Jain et al. 2015. Autism occurrence by MMR vaccine status among US children with older siblings with and without autism. JAMA 313:1534–1540
- Jafari et al. 2017. The association between mercury levels and autism spectrum disorders: A systematic review and meta-analysis. Journal of Trace Elements in Medicine and Biology 44:289–297.
- James 2004. Metabolic biomarkers of increased oxidative stress and impaired methylation capacity in children with autism. Am J Clin Nutr 80:1611–1617
- James et al. 2005. Thimerosal neurotoxicity is associated with glutathione depletion: protection with glutathione precursors. NeuroToxicol 26:1–8
- James et al. 2006. Metabolic endophenotype and related genotypes are associated with oxidative stress in children with autism. American Journal of Medical Genetics B 141B:947–956.
- Jefferson et al. 2003. Unintended events following immunization with MMR: a systematic review. Vaccine 21:3954–3960
- Kanner. 1943. Autistic disturbances of affective contact. Nervous Child 2:217–250
- Kawashima et al. 2000. Detection and sequencing of measles virus from peripheral mononuclear cells from patients with inflammatory bowel disease and autism. Dig Dis Sci 45:723–729
- Kawashti. 2006. Possible immunological disorders in autism: concomitant autoimmunity and immune tolerance. Egypt J Immunol 13:99–104
- Kaye et al. 2001. Mumps, measles, and rubella vaccine and the incidence of autism recorded by general practitioners: a time-trend analysis. West J Med 174387–390
- Kempuraj. 2010. Mercury induces inflammatory mediator release from human mast cells. J Neuroinflammation 7:20
- Kern and Jones. 2006. Evidence of toxicity, oxidative stress, and neuronal insult in autism. J Toxicol Environ Health B Crit Rev 9:485–499
- Khan et al. 2013. Slow CCL2-dependent translocation of biopersistent particles from muscle to brain. BMC Med 11:99
- Khaled et al. 2016. Altered urinary porphyrins and mercury exposure as biomarkers for autism severity in Egyptian children with autism spectrum disorder. Metabolic Brain Disease 31:1419–1426.
- King et al. 2013. Topoisomerases facilitate transcription of long genes linked to autism. Nature 501:58–62
- Klein and Diehl. 2004. Relationship between MMR vaccine and autism. Annals of Pharmacotherapy 38:1297–1300
- Leviton et al. 2018. The risk of neurodevelopmental disorders at age 10 years associated with blood concentrations of interleukins 4 and 10 during the first postnatal month of children born extremely preterm. Cytokine 110:181–188.
- Li et al. 2014. Transcriptomic analyses of neurotoxic effects in mouse brain after intermittent neonatal administration of thimerosal. Toxicol Sci 139:452–465
- Li et al. 2018. Blood Mercury, Arsenic, Cadmium, and Lead in Children with Autism Spectrum Disorder. Biological Trace Element Research 181:31–37.
- Lukiw et al. 2005. Nanomolar aluminum induces pro-inflammatory and pro-apoptotic gene expression in human brain cells in primary culture. J Inorg Biochem 99:1895–1898
- Lyons-Weiler 2018. Autism is an Acquired Cellular Detoxification Deficiency Syndrome with Heterogeneous Genetic Predisposition. Autism Open Access 8:1
- Madsen et al. 2002. A population-based study of measles, mumps, and rubella vaccination and autism. New England Journal of Medicine 347:1477–1482
- Madsen et al. 2003. Thimerosal and the occurrence of autism: negative ecological evidence from Danish population-based data. Pediatrics 112:604–606
- Makela et al. 2002. Neurologic disorders after measles-mumps-rubella vaccination. Pediatrics 110:957–963.
- Margaret et al. 2014. Safety of vaccines used for routine immunization of US children: a systematic review. Pediatrics 134:1–13
- RETRACTED Mawson et al. 2017a. Pilot comparative study on the health of vaccinated and unvaccinated 6- to 12- year old U.S. children. Journal of Translational Science 3. (see retraction watch)
- Mawson et al. 2017b. Preterm birth, vaccination and neurodevelopmental disorders: a cross-sectional study of 6- to 12-year-old vaccinated and unvaccinated children. Journal of Translational Science 3.
- Migdal et al. 2010. Sensitization effect of thimerosal is mediated in vitro via reactive oxygen species and calcium signalling. Toxicol. 274:1–9
- Minami et al. 2010. Induction of metallothionein in mouse cerebellum and cerebrum with low-dose thimerosal injection. Cell Biol Toxicol 26:143–152
- Mizejewski et al. 2013. Newborn screening for autism: in search of candidate biomarkers. Biomarkers in medicine 7:247–260.
- Molina and Shoenfeld 2005. Infection, vaccines and other environmental triggers of autoimmunity. Autoimmunity 38:235–245
- Mold et al. 2018. Aluminium in brain tissue in autism. Journal of Trace Elements in Medicine and Biology 46:76–82.
- Morgan et al. 2010. Microglial Activation and Increased Microglial Density Observed in the Dorsolateral Prefrontal Cortex in Autism. Biological Psychiatry 68:386–376.
- Morris et al. 2017a. The putative role of environmental aluminium in the development of chronic neuropathology in adults and children. How strong is the evidence and what could be the mechanisms involved? Metabolic Brain Disease 32:1335–1355.
- Morris et al. 2017b. The Putative Role of Environmental Mercury in the Pathogenesis and Pathophysiology of Autism Spectrum Disorders and Subtypes. Molecular Neurobiology 55: 4834–4856
- Mumper. 2013. Can awareness of medical pathophysiology in autism lead to primary care autism prevention strategies? N A J Med Sci 6:134–144
- Naik et al. 2011. A Study of Nuclear Transcription Factor-Kappa B in Childhood Autism. 6:e19488
- Namvarpour et al. 2018. Protective role of alpha-lipoic acid in impairments of social and stereotyped behaviors induced by early postnatal administration of thimerosal in male rat. Neurotoxicology Teratology 67:1–9.
- Nataf. 2006. Porphyrinuria in childhood autistic disorder: implications for environmental toxicity. Toxicol Appl Pharmacol 2006:99–108
- Neustadt and Pieczenik. 2007. Heavy-metal toxicity – with emphasis on mercury. IMCJ 6:26–32
- Nevison 2014. A comparison of temporal trends in United States autism prevalence to trends in suspected environmental factors. Envrion Health 13:73
- Nevison et al. 2017. Diagnostic Substitution for Intellectual Disability: A Flawed Explanation for the Rise in Autism. Journal of Autism and Developmental Disorders 47:2733–2742.
- Nevison et al. 2018. California Autism Prevalence Trends from 1931 to 2014 and Comparison to National ASD Data from IDEA and ADDM. Journal of Autism and Developmental Disorders 48:4103–4117.
- Nordahl et al. 2011. Brain enlargement is associated with regression in preschool-age boys with autism spectrum disorders. Proceedings of the National Academy of Sciences 108:20195–20200.
- Olczak et al. 2009. Neonatal administration of a vaccine preservative, thimerosal, produces lasting impairment of nociception and apparent activation of opioid system in rats. Brain Research 1301:143–151
- Olczak et al. 2010a. Lasting neuropathological changes in rat brain after intermittent neonatal administration of thimerosal. Folia Neuropathologica 48:258–269.
- Olczak et al. 2010b. Neonatal administration of thimerosal causes persistent changes in mu opioid receptors in the rat brain. Neurochem Res 35:1840–1847
- Olczak et al. 2011. Persistent behavioral impairments and alterations of brain dopamine system after early postnatal administration of thimerosal in rats. Behavioral Brain Research 30:107–118.
- Oliveira. 2007. Epidemiology of autism spectrum disorder in Portugal: prevalence, clinical characterization, and medical conditions. Dev Med Child Neurol 49:726–733
- Palmer et al. 2006. Environmental mercury release, special education rates, and autism disorder: an ecological study of Texas. Health Place 12:203–209
- Palmer et al. 2008. Proximity to point sources of environmental mercury release as a predictor of autism prevalence. Health Place 15:18–24
- Parker et al. 2004. Thimerosal-containing vaccines and autistic spectrum disorder: A critical review of published original data. Pediatrics 114:793–804
- Petrik. 2007. Aluminum adjuvant linked to Gulf War illness induces motor neuron death in mice. Neuromolecular Med 9:83–100
- Poling. 2006. Developmental regression and mitochondrial dysfunction in a child with autism. J Child Neurol 21:170–172
- Price et al. 2010. Prenatal and infant exposure to thimerosal from vaccines and immunoglobulins and risk of autism. Pediatrics 16:656–64
- Ratajczak. 2011. Theoretical aspects of autism: causes–a review. J Immunotoxicol 8:68–79
- Rice. 1989. Brain and tissue levels of mercury after chronic methylmercury exposure in the monkey. J Toxicol Environ Health 27:189–198
- Rimland and McGinnis. 2002. Vaccines and autism. Laboratory Medicine 9:708–717
- Risher and Tucker 2017. Alkyl Mercury-Induced Toxicity: Multiple Mechanisms of Action. Reviews of Environmental Contamination and Toxicology 240:105–149.
- Robertson et al. 2015. Reduced GABAergic action in the autistic brain. Curr Biol 26:80–85
- Rooney. 2014. The retention time of inorganic mercury in the brain—a systematic review of the evidence. Toxicol Appl Pharmacol 274:425–435
- Rossignol and Bradstreet. 2008. Evidence of mitochondrial dysfunction in autism and implications for treatment. Am J Biochem Biotechn 4:208–217
- Rossignol and Frye. 2012. Mitochondrial dysfunction in autism spectrum disorders: a systematic review and meta-analysis Molecular Psychiatry 17:290–314
- Rubenstein et al. 2015. A review of the differences in developmental, psychiatric, and medical endophenotypes between males and females with autism spectrum disorder. J Dev Phys Disabil 27:119–139
- Russo et al. 2018. Modeling the Interplay Between Neurons and Astrocytes in Autism Using Human Induced Pluripotent Stem Cells. Biological Psychiatry 83:569–578.
- Rutter. 2005. Incidence of autism spectrum disorders: changes over time and their meaning. Acta Paediatr 94:2–15
- Sajdel-Sulkowska et al. 2008. Oxidative stress in autism: elevated cerebellar 3-nitrotyrosine levels. Am J Biochem Biotechnol 4:73–84
- Schechter and Grether. 2008. Continuing increases in autism reported to California’s developmental services system: mercury in retrograde. JAMA Physch 65:19–24
- Schulz. 2000. Glutathione, oxidative stress and neurodegeneration. Eur J Biochem. 267:4904–4911
- Scott et al. 2017. Clinical clues for autoimmunity and neuroinflammation in patients with autistic regression. Developmental Medicine and Child Neurology 59:947–951.
- Seneff et al. 2012. Empirical data confirm autism symptoms related to aluminum and acetaminophen exposure. Entropy 4:2227–2253
- Shandley and Austin. 2011. Ancestry of pink disease (infantile acrodynia) identified as a risk factor for autism spectrum disorders. J Toxicol Environ Health A 74:1185–1194
- Sharpe et al. 2012. Thimerosal-derived ethylmercury is a mitochondrial toxin in human astrocytes: possible role of fenton chemistry in the oxidation and breakage of mtDNA. J Toxicol 373678
- Sharpe et al. 2013. B-Lymphocytes from a population of children with autism spectrum disorder and their unaffected siblings exhibit hypersensitivity to thimerosal. J Toxicol 2013:801517
- Shaw and Tomljenovic. 2013a. Administration of aluminium to neonatal mice in vaccine-relevant amounts is associated with adverse long term neurological outcomes. J Inorg Biochem 128:237–244
- Shaw and Tomljenovic. 2013b. Aluminum in the central nervous system (CNS): toxicity in humans and animals, vaccine adjuvants, and autoimmunity. Immun Res 56:304–316
- Shaw et al. 2014a. Aluminum-induced entropy in biological systems: Implications for neurological disease. J Toxicol 2014:491316
- Shaw et al. 2014b. Etiology of autism spectrum disorders: Genes, environment, or both? OA Autism 2:11
- Sienkiewicx et al. 2012. Neurological adverse events following vaccination. Prog health Sci 2:129–141
- Singh. 2009. Phenotypic expression of autoimmune autistic disorder (AAD): A major subset of autism. Ann Clin Psychiat 21:148–161
- Singh et al. 1998. Serological association of measles virus and human herpesvirus-6 with brain autoantibodies in Autism. Clin Immunol Immunopathol 89:105–108
- Singh et al. 2002. Abnormal measles-mumps rubella antibodies and CNS autoimmunity in children with autism. J Biomed Sci 9:359–364
- Smeeth et al. 2004. MMR vaccination and pervasive developmental disorders: a case-control study. Lancet 364:963–969
- Stratton et al. (eds). 2011. Adverse Effects of Vaccines: Evidence and Causality. Committee to Review Adverse Effects of Vaccines, Institute of Medicine. Washington (DC): National Academies Press (US)
- Sun et al. 2018. Early seizures prematurely unsilenced auditory synapses to disrupt thalamocortical critical period plasticity. Cell Reports 23:2533–2540
- Richler et al. 2006. Is there a ‘regressive phenotype’ of autism spectrum disorder associated with measles-mumps-rubella vaccine? A CPEA study. J Autism Dev Disord 36:299–316
- Ryu et al. 2017. Associations of prenatal and early childhood mercury exposure with autistic behaviors at 5 years of age: The Mothers and Children’s Environmental Health (MOCEH) study. Science of the Total Environment 605-606: 257.
- Stajich et al. 2000. Iatrogenic exposure to mercury after hepatitis B vaccination in preterm infants. J Pediatr 136:676–681
- Stamova et al. 2009. Correlations between gene expression and mercury levels in blood of boys with and without autism. Neurotox Res 19:31–48
- Sulkowski et al. 2012. Maternal thimerosal exposure results in aberrant cerebellar oxidative stress, thyroid hormone metabolism, and motor behavior in rat pups; sex- and strain-dependent effects. Cerebellum 11:575–586
- Taylor et al. 1999. Autism and measles, mumps, and rubella vaccine: no epidemiological evidence for a causal association. Lancet 353: 2026–2029
- Taylor. 2006. Vaccines and the changing epidemiology of autism. Child Care Health Dev. 32:511–519
- Taylor et al. 2014. Vaccines are not associated with autism: and evidence-based meta-analysis of case-control and cohort studies. Elsevier 32:3623-3629
- Tomljenovic and Shaw. 2011. Do aluminum vaccine adjuvants contribute to the rising prevalence of autism? J Inorg Biochem 105:1489–1499
- Tomljenovic and Shaw. 2012. Mechanisms of aluminum adjuvant toxicity and autoimmunity in pediatric populations. Lupus 21:223–230
- Tsumiyama et al. 2009. Self-organized criticality theory of autoimmunity. PLoS ONE 4:e8382
- Uno et al. 2015. Early exposure to the combined measles-mumps-rubella vaccine and thimerosal-containing vaccines and risk of autism spectrum disorder. Vaccine 33:2511–2516
- Uchiyama et al. 2007. MMR-vaccine and regression in autism spectrum disorders: negative results presented from Japan. J Autism Dev Disord 37:210–217
- Vargas. 2005. Neuroglial activation and neuroinflammation in the brain of patients with autism. Ann Neurol 57:67–81
- Vasquez 2017. Biological plausibility of the gut-brain axis in autism. Annals of the New York Academy of Sciences 1408:5–6.
- Verstraeten et al. 2003. Safety of Thimerosal-Containing Vaccines: A two-phased study of computerized health maintenance organization databases. Pediatrics 112:1039–1048
- Verstraeten et al. 2014. Increased risk of developmental neurologic impairment after high exposure to thimerosal-containing vaccine in first month of life. Proceedings of the Epidemic Intelligence Service Annual Conference 49
- Vestergaard et al. 2004. MMR vaccination and febrile seizures: evaluation of susceptible subgroups and long-term prognosis. JAMA 292:351–357
- Waly et al. 2004. Activation of methionine synthase by insulin-like growth factor-1 and dopamine: a target for neurodevelopmental toxins and thimerosal. Mol Psychiatry 9:358–70
- Walker et al. 2006. Cultured lymphocytes from autistic children and non-autistic siblings up-regulate heat shock protein RNA in response to thimerosal challenge. Neurotoxicology 27:685–692
- Walker et al. 2013. Identification of unique gene expression profile in children with regressive autism spectrum disorder (ASD) and ileocolitis. PLoS ONE 8: e58058
- Wang et al. 2018. IL-4 mediates the delayed neurobehavioral impairments induced byneonatal hepatitis B vaccination that involves the down-regulation of the IL-4 receptor in the hippocampus. Cytokine 110:137–149.
- Weizman et al. 1982. Abnormal immune response to brain tissue antigen in the syndrome of autism. Am J Psychiatry 139:1462-1465
- Werner and Dawson. 2005. Validation of the phenomenon of autistic regression using home videotapes. Arch Gen Psychiatry 62:889–895
- Wilson et al. 2011. Adverse events following 12 and 18 month vaccinations: a population-based, self-controlled case series analysis. PLoS ONE 6:e27897
- Windham et al. 2006. Autism spectrum disorders in relation to distribution of hazardous air pollutants in the San Francisco bay area. Environ Health Perspect 114:1438–1444
- Woods et al. 2010. Urinary porphyrin excretion in neurotypical and autistic children. Environ Health Perspect 118:1450–1457
- Wong et al. 2014. Methylomic analysis of monozygotic twins discordant for autism spectrum disorder and related behavioural traits. Molecular Psychiatry 19:495–503.
- Wu et al. 2008. Thiol-modulated mechanisms of the cytotoxicity of thimerosal and inhibition of DNA topoisomerase II alpha. Chem Res Toxicol 21:483–493
- Yasuda and Tsutsui. 2013. Assessment of infantile mineral imbalances in autism spectrum disorders (ASDs). Int J Environ Res Public Health 10:6027–6043
- Yassa. 2014. Autism: a form of lead and mercury toxicity. Environ Toxicol Pharmacol. 38:1016–1024
- Yel. 2005. Thimerosal induces neuronal cell apoptosis by causing cytochrome c and apoptosis-inducing factor release from mitochondria. Int J Mol Med 16:971–977
- Young et al. 2008. Thimerosal exposure in infants and neurodevelopmental disorders: an assessment of computerized medical records in the Vaccine Safety Datalink. J Neurol Sci 271:110–118
- Young et al. 2010. Porphyrinuria in Korean children with autism: correlation with oxidative stress 73:701–710
- Young et al. 2011. Aberrant NF-KappaB expression in autism spectrum condition: A mechanism for neuroinflammation. Front Psychiatry 2:27
- Zhang et al. 2012. Risk factors for autistic regression: results of an ambispective cohort study. J Child Neurol. 27:975–981
- Zhang et al. 2014. Thioredoxin: A novel, independent diagnosis marker in children with autism. Int J Dev Neurosci 40:92–66

Fantastic effort, this is golden!
LikeLike
Hear, hear! And it is almost embarrassing that apparently so few people took the effort to read it and rate it … What is said here, should be mandatory literature for anyone talking about vaccines out on InstaFaceTwitWhatever.
LikeLike
Vaccines. Don’t. Cause. Autism.
LikeLike
I’d press like a dozen times. Thanks for doing this.
My favourite part: “Of the 160 papers in the lists, there were 33 that were not about autism and 82 that were not about vaccines!”
That reminds me of the lists of papers climate deniers put together. As soon as you start looking into them you find just how few of them actually support their position.
LikeLike